
How can the toughest problems of urban life be addressed in a serious, sustained way? The purpose of this series, which began with “What To Do (and Not To Do) About Subway Safety” and will continue with installments on disorder, policing and other topics, is to deliver to policymakers the best ideas distilled into steps that can be taken now and longterm changes that must undergird sustained achievement.
We assembled prominent practitioners and researchers to discuss the complicated problem of individuals who are unhoused and living with serious mental illness (SMI) and drug addiction on New York City’s streets and subways. In this issue, more than any other we have examined, the data are sparse and atomized, and the evidence of “what works” is frail. But policymakers have no choice but to act even when there is no randomized controlled trial to guide them. Here, we relied on the deep experience of those addressing these issues to fashion practical recommendations — the repeating theme is that for a solution to endure, the City must steel itself to synthesize data and test results.
This document contains our chief recommendations. It is supplemented by three companion papers: a look at what the data tell us and fail to tell us about this population, a detailed description of the way the system currently works and a look at how other large cities handle these problems.
Our deep gratitude goes to the many people who helped shape these recommendations. Many of them are listed at the end of this document. We also extend special thanks to the Achelis and Bodman Foundation, Arnold Ventures, the Harry Frank Guggenheim Foundation, the Public Welfare Foundation, the Charles H. Revson Foundation, the Teagle Foundation and the Tow Foundation, who are helping to support Vital City. We appreciate the work others throughout the city are doing to assemble and advance similar recommendations, including The Collaborative on Housing for Health, and consider our work complementary to theirs. While we make recommendations here, they are in part based on and honor the hard work of public servants who grapple with these enormously complex problems every day.
The Problem To Be Solved
Of all the hard urban problems, none tests New York’s capacity for effective governance quite like this one: people occupying public places while living with SMI, addiction and other maladies. It is a problem that touches first principles — how government cares for vulnerable people in distress and how to ensure public spaces remain safe and accessible for the public’s use. And it exposes the limits of government knowledge, coordination and intervention. New York lacks a reliable, citywide picture of who these New Yorkers are, what conditions they live with, who connects with them for support and which interventions actually change their life course for the better. Policymakers, advocates and the broader public argue about whether this is a public health problem or a public safety problem — when, in truth, it is both.
Layered atop that is a hard question of agency: When illness and addiction distort a person’s judgment, obscure their insight or diminish their ability to acknowledge the problems they face, how should the City balance a person’s autonomy with its obligation to protect life and the shared use of public space? Unlike challenges that respond to standardized playbooks, these individuals’ needs shift quickly. Progress is nonlinear, and durable results hinge on sustained work that, to be effective, must be bespoke to the particular condition of each person. All of those uncertainties are further aggravated by the loose relationship that government and other entities often have to the evidence — such as it is — that might guide government actions.
People who are homeless have a right to occupy public space, like anyone else. But as with every person, there are limits on how public space is shared. They do not have a right to create encampments, to use drugs in public view or to harass others. Nor do they have the right to violate the rules of the subway system, which is primarily for transit. When public places become places where crises routinely play out, other New Yorkers can feel uneasy or unsafe, and in some cases, there is genuine danger — to these vulnerable individuals themselves and to the wider public.
The City, including in this last administration, has tried many things over several decades. New York City, with support from New York State and federal partners, spends billions annually across a sprawling range of programs: street outreach and mobile intervention; 911 and 311 crisis response; inpatient and step-down care; a vast, specialized shelter system; low-barrier options, including Safe Havens and stabilization beds; jail and hospital reentry services; and supportive and affordable housing. A glossary of many of these terms is part of our companion document, “How the System Works (and Doesn’t).” Recently passed legislation codifies the criteria for involuntary removal from the street, and both the City and the State have expanded the use of outreach teams comprising police and clinicians.
Still, New Yorkers, City agencies, nonprofits and the myriad who work every day on this issue report a common frustration: The same individuals cycle through subways, ERs, courts, incarceration, shelters and streets, in a seemingly never-ending churn. New Yorkers seem to be paying too much for motion and not enough for durable results.
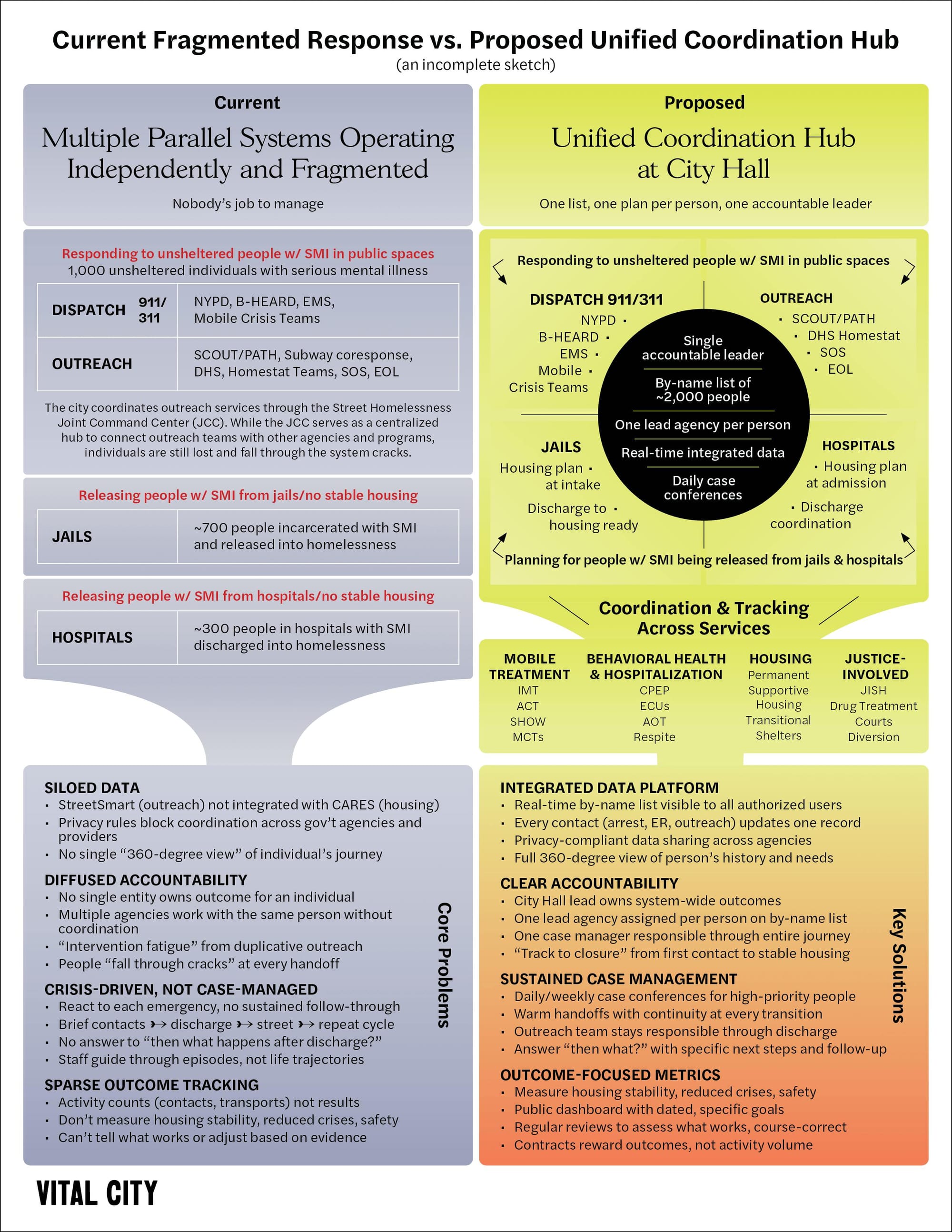
Two problems, in particular, plague the efforts to address these hard problems. First, no one “owns” the issue — so no one is held accountable when an individual isn’t successfully linked with stable housing and care. Second, the fragmentation of the efforts — data, accountability, goals — means that it is oriented toward crisis, not durable solutions. There are many committed individuals and groups serving and interacting with unhoused people, including those living with mental illness, but coordination and accountability are diffuse or nonexistent. But the system is organized mainly by agency, geography and category of service rather than by individuals in need, and is most often mobilized in response to crisis. Successful follow-through focused on the needs of a particular person from day to day, much less month to month, is rare.
Mayor-elect Zohran Mamdani plans to establish a Department of Community Safety to coordinate outreach and response to this vulnerable population. Our experience suggests that the success or failure of the City’s engagement with unstable homeless New Yorkers will not hinge on whether a new department is added to the current mix of many agencies working in this space. Rather, the next mayor’s broader management strategy will be crucial to whether a new department adds value or becomes yet another layer and level of siloed bureaucracy.
To ensure operations and implementation are successful, Mamdani will need to establish, for all City government, a clear goal and focus to achieve measurable progress in this space. One place within the government — we recommend the Mayor’s Office for having the authority and span sufficient to coordinate multiple entities — must have the mandate, accountability, data and resources to ensure that each person who is in crisis has the support through and beyond crisis to get to treatment and housing placement. The shorthand for this accountability is: “Who is ultimately responsible to the mayor for real and enduring progress in ensuring housing and treatment for this vulnerable population?” As we detail below, this will require a major effort by the City to assemble information about people and how they are served and to steel itself to learn relentlessly what works and what doesn’t.
Based on our analysis of successful programs from other states and lessons learned from past administrations in New York City, the following recommendations focus on addressing the needs of the relatively small group of unsheltered individuals who present a danger to themselves or others, either through mental instability or debilitating addiction. By staying focused and filling the service gaps for this most complicated population, the City will necessarily strengthen and improve the system for all homeless people living with mental illness and/or a substance use disorder.
To ensure this goal is met, services must no longer be siloed by agency and geography, but rather structured such that government and nonprofits are assigned to individuals and tasked with addressing their complex needs, across bureaucratic barriers and over time. Providers should be measured by their results, and, backlighting everything, the City should be fiercely committed to continually evaluating effectiveness. This is necessary for making nimble operational decisions regarding what to replicate and what to correct. And, for the long haul, the City must also commit to put in place a stable and durable policy to change conditions for the better. There must be a common agreement both that public places are for public use, and that the aim is ultimately to ensure each unsheltered person is housed and supported with the services that will make their lives stable and safe.
How the System Works (or Doesn’t)
On any given night, about 4,000 people are living on the streets and subways in New York City. Perhaps half of them — there is no perfect estimate — live with SMI, addiction and other profound problems. Over decades, the City has built a vast web of public and nonprofit providers to reach, house and treat this population.
An incomplete catalog: Teams of outreach workers from organizations like the Bowery Residents’ Committee and the Center for Urban Community Services fan out daily. Police officers are often the first to encounter people in desperation or outright crisis; under the law, they are empowered to take individuals to hospitals, where doctors and nurses determine if they need psychiatric care and judges may order involuntary commitment.
A relatively new innovation, the co-response team, which consists of police and clinicians, seeks to make informed judgments about people’s needs and connect them to appropriate services. In the past few years, there has been additional focus on “alternative response,” in which civilians engage with people in need on the street without the police. Intensive Mobile Treatment (IMT) teams work with the highest-need people who have substantial criminal justice involvement. Temporary shelter placements and supportive housing — apartments with a wide array of wraparound help to address needs — are coordinated through the Department of Homeless Services (DHS) and other agencies.
Prosecutors and courts get involved when people are accused and convicted of crimes. Court-ordered evaluations, known as 730 exams, provide an early opportunity to examine an individual for fitness to proceed and to route a person to treatment if they are found incapacitated. While in custody, those living with SMI — about a fifth of the jail population at any given time — can be housed in specialized units. Upon release, reentry programs are available to connect individuals to treatment, housing and other services. If convicted of a crime and transferred to State custody, there is a range of treatment, specialized beds and units for individuals with SMI.
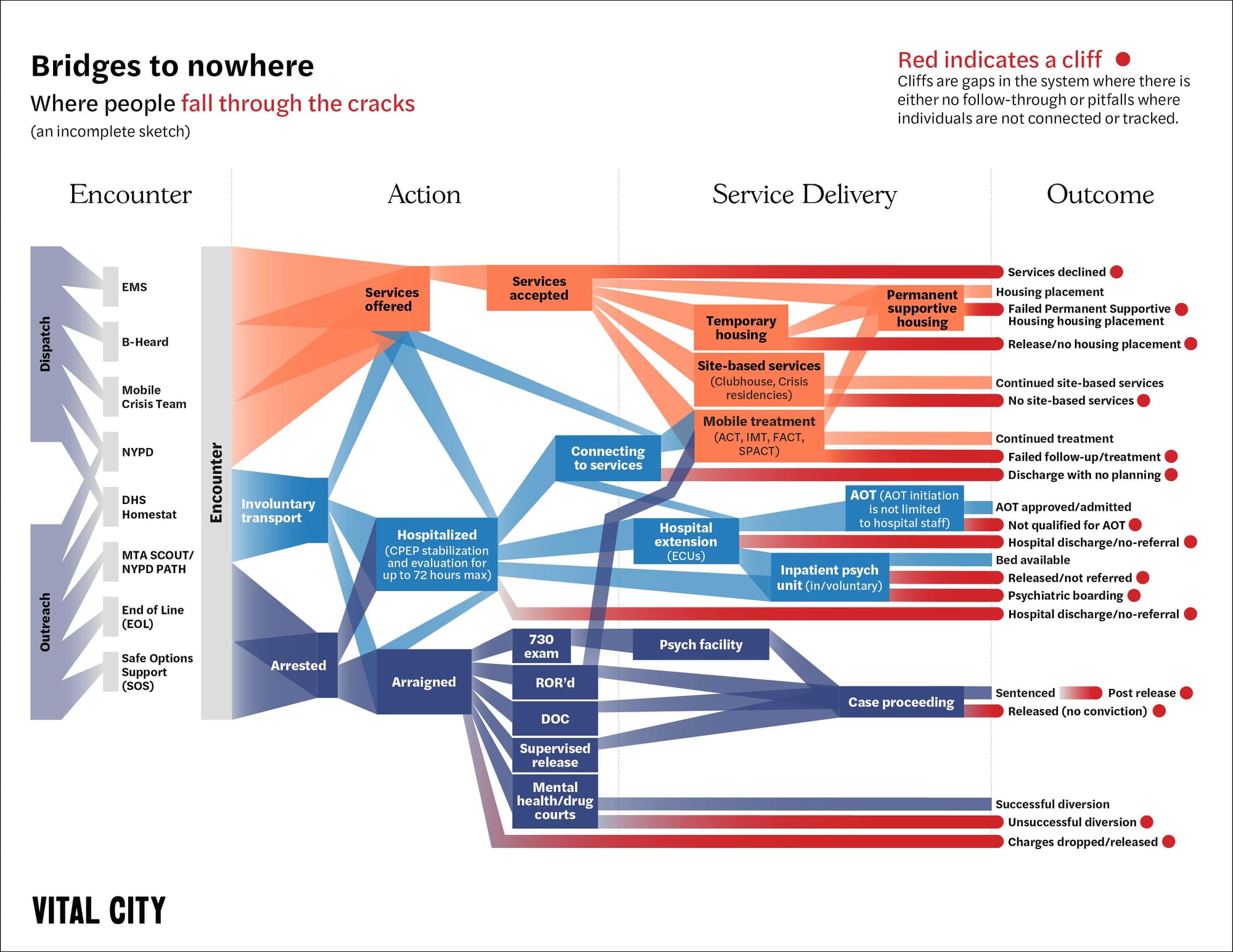
The result is an elaborate and poorly coordinated ecosystem that costs taxpayers billions each year. For policymakers and the public alike, keeping track of the panoply of programs and acronyms can be dizzying. Those wishing to understand how these programs fit together can start with Vital City’s crash course here.
For every attempt to engage, for every handoff from one nonprofit or government agency to another, there is a potential cliff — where people in need fail to get the help they need, further aggravating the likelihood of crisis.
Principles for Action
- Affirm and enforce that public spaces are for public purposes. Streets, subways and parks are shared civic resources. When they are used in ways that block access, compromise safety or depart from their intended function, the City has an obligation to ensure their fair, cooperative use.
- Set a citywide goal of providing stable housing and care for each person in distress, recognizing that attention must be sustained beyond crisis. People who are unhoused and suffering from mental illness and other maladies should have access to permanent housing and care suited to their needs for as long as necessary to achieve stability.
- Ensure clear responsibility for meeting goals and relentlessly focus on learning what works and what doesn't. Today, accountability regarding this population is diffuse and in some cases nonexistent. Responsibility for results must be the hallmark of the system.
- Coordinate across systems with contracts oriented around results, not activity. All activity should be oriented toward common goals with publicly available metrics that measure results, not simply activity.
- Lead with health, support with safety. When a person is in psychiatric distress, the response should be guided by health professionals, with police ready to ensure safety and legitimacy when needed. Success depends on effective coordination and cooperation.
Summary of Recommendations
1. Affirm and enforce public space norms while unifying all City action around stable housing and care.
The City should consistently enforce rules that keep public spaces usable while ensuring every removal is paired with concrete offers of treatment, shelter and a pathway to permanent housing.
2. Put one accountable City Hall leader in charge of the entire system.
A single mayoral authority should coordinate all agencies, data, contracts and actions across health, housing, transit, police and courts to focus on outcomes rather than activity.
3. Treat housing as the essential foundation of stabilization.
The City must rapidly scale and streamline direct placements into supportive or hybrid housing-with-services, removing bureaucratic barriers and prioritizing people with the highest needs.
4. Focus outreach, treatment and enforcement on the small group driving the most instability.
Using integrated justice, health and homelessness data, the City should concentrate intensive treatment, housing and supervision on the highest-risk individuals and locations.
5. Use involuntary removals strategically and always as a gateway to sustained care.
When danger is clear, involuntary transport and psychiatric treatment should be used more consistently and should always be connected to continuous outreach, treatment and housing rather than cycling people back to the street.
6. Reform contracts and rationalize hundreds of millions of dollars in spending around outcomes, not activities.
The City should pay providers on time, consolidate fragmented funding, track costs per person across systems and shift to outcome-based contracting tied to durable stability.
7. Follow the evidence and rigorously evaluate every strategy.
The City should fast-track pilots, measure outcomes across systems, fund independent evaluations and stop or scale programs based strictly on demonstrated results.
What not to do
Avoid punitive or symbolic actions — like police-only strategies or encampment sweeps without housing — and stop expanding unevaluated programs or treating all cases the same. Instead, tailor interventions and measure outcomes.
Recommendations in detail
1. Affirm and enforce that public spaces are for public purposes while unifying City action under a common goal of providing stable housing with necessary supports.
The City must not stand by while people in active psychiatric or substance use crisis, or those who are teetering on the verge of crisis, unravel in public view. This is both because of the well-being of the person in crisis and because of the threat or perceived threat presented, both of which are corrosive to the fabric of the city. The numerous agencies and entities involved in this issue must operate in unison under a common goal that will orient and direct action and provide for sustained attention for those in need. That common goal is to provide stable housing for each person along with the tailored services needed to maintain stability. Specifically, the City should:
- Codify the principle in agency protocols. City and State agencies like the NYPD, DHS, Department of Parks and Recreation and Metropolitan Transportation Authority (MTA) should make clear in their training and operating guidelines that public spaces are not to be used as encampments, sites of open-air drug use or places where people remain in active psychiatric distress. Frontline staff should be directed that behavior cannot be ignored when it violates the law.
- Effect removals from the subways and other public spaces and ensure consistent, coordinated outreach connecting people to services. The first set of recommendations in Vital City's "What To Do (and Not To Do) About" series focused on subway safety and made clear that police and outreach workers should "remove from the system those who violate the rules or present risks." We second that here. The subway's rules are designed to ensure New Yorkers can travel efficiently and safely. Aboveground, the rules for removal may vary by location. But in all cases, the goal should be to prevent deterioration in public and connect people with necessary treatment and housing.
- Set clear expectations through public messaging. The City should mount a campaign to reinforce that streets and especially subways are not acceptable living spaces and to highlight the help available. This can acknowledge and reinforce these important norms and invite the public to report serious safety or health concerns via 311, helping to identify locations where conditions are deteriorating and outreach is urgently needed.
- Pair removals with advance notice whenever feasible, and with concrete offers of care aimed at permanent housing and services. Enforcement alone is insufficient if it simply displaces the person. Every removal should lead to services oriented toward securing housing, treatment and other help. This is a tall order. But beginning with the relatively small number of highest-acuity individuals can help the City build the staffing, coordination and operational pathways needed for a more organized system.
2. Organize people, programs, access to data and focus on results under a single City Hall lead.
New York needs a single accountable leader at City Hall with the power, authority and means to oversee the response to people living on the streets beset with SMI and drug addiction. Diffuse accountability produces inconsistent standards and misaligned incentives as agencies optimize their own workloads instead of outcomes for the person or the community block. This leader must control budgets and contracts and have the authority to compel privacy-compliant data sharing. They should also oversee an operational hub that assigns a lead agency to each person and formalizes State-City coordination. With that mandate, the City can measure what matters and own results rather than activities.
We recognize that this reorganization is no small task, but the current arrangement has not worked. As structured, it cannot succeed. Much work has been done by those involved in these issues every day, and informal working groups with deep knowledge of the system abound. Specifically, the City should:
- Designate one Mayor's Office official as the chief City official responsible for this population. This office should convene all relevant entities, set goals and expectations and ensure coordination. It should also map the web of interactions across systems and set clear accountability standards for outreach, follow-up, housing and treatment. This coordinating authority must sit in the Mayor's Office so it can direct agencies, ensure goals are met, mobilize resources to support implementation and have the authority to coordinate effectively with state agencies (e.g. the MTA, the New York State Office of Mental Health and the New York State Office of Addiction Services and Supports, among others). Mayor-elect Mamdani's proposed Department of Community Safety would house some (perhaps all) of the outreach and response teams, but it does not solve the coordination and direction problem — which will remain multiagency by definition, necessarily involving the Department of Health and Mental Hygiene (DOHMH), NYC Health + Hospitals (H+H), DHS, the NYPD and other City departments, as well as offices, departments and agencies at the State and federal levels.
- Integrate justice, health and homelessness data under the City's Center for Innovation through Data Intelligence as the backbone. The City should build a single, privacy-compliant, by-name picture that matches arrests, hospitalizations, involuntary transports, Medicaid claims and outreach contacts to flag high-risk individuals in real time. Incorporating justice data streams, this can help close the well-documented divide between public health and criminal justice systems, much of it driven by tradition and mistrust rather than law. Such a platform can vastly improve and inform outreach and intervention efforts.
- Hold regular multiagency "case conferences." The individual in charge of coordination should convene daily or weekly meetings where frontline teams and supervisors discuss the highest-priority individuals and assign tasks. No two individuals present precisely the same challenge. This tight feedback loop mirrors successful models such as veteran homelessness case conferencing, New York City's gun violence reduction strategy, the "Top 50" lists and multidisciplinary task forces elsewhere in the state. Public safety risk should be included in considering the highest-priority individuals.
- Aggregate and analyze knowledge. While individual cases must be managed better, the City simultaneously needs a much clearer, 35,000-foot view of the population as a whole. It should build a single, integrated picture of the problem across agencies. It should establish a comprehensive assessment of the correct alignment of resources needed to achieve the vision of overcoming street homelessness by mapping the churn and flow of individuals and their needs. And for public consumption, it should publish the "known unknowns" and a plan to close system gaps.
- Reorient contracts to ensure their specifications are based on individuals and outcomes. The City's current contracting with nonprofits is siloed by agency and geography, creating a tangled web of bureaucracies. Dozens of nonprofits contract across City agencies, spending many hundreds of millions of dollars annually. These organizations can hold multiple contracts with single agencies and often contract with several agencies simultaneously. Contracting should be restructured and sufficiently funded so that payments are based on outcomes, not inputs, and so that organizations are assigned to individuals and not arbitrary geographic or bureaucratic realms. These outcomes should include but not be limited to: longitudinal health outcomes, justice-system involvement and housing placements.
- Explore other contracting reforms to improve coordination and accountability. Contracts with providers should require shared data systems and standardized consent processes to enable responsible information exchange among providers. Outreach areas should be aligned geographically to reduce overlap and strengthen accountability and follow-up.
- Compel privacy-compliant data sharing. Building on existing platforms such as the "Top 50" lists of especially troubled individuals and DHS' StreetSmart, intended to be a coordinated tracking system, the City must compel more privacy-compliant data sharing. City Hall should identify gaps in data sharing and clarify whether they stem from legal, policy or technical barriers. Where information is incomplete or siloed, agencies should execute new data-sharing agreements or pursue legislative remedies as needed to ensure that outreach, hospital and housing systems operate from a shared picture of each person's status and needs. For example, the Times Square Alliance has proposed reforms that let multidisciplinary teams share information across health, housing and safety systems while maintaining confidentiality. Modeled on California's AB 210, such legislation would authorize controlled data sharing among qualified providers and create the foundation for a unified outreach and care system.
- Focus on the highest-need people first in a tightly scoped 100-day pilot. Some have suggested that such a pilot should initially be constrained geographically to a single precinct or community district — plus nearby transit hubs. Others note the limitations of a geographically bounded pilot because the issues cross borders. The City should choose whichever model they can use best to test a fully coordinated, data-driven approach to address unsheltered homelessness. Empower a City Hall lead and on-the-ground operations manager to unify all outreach, clinical, housing and enforcement efforts within clear geographic boundaries. Establish daily field briefings, weekly interagency case conferences and monthly strategic reviews to align actions and remove system barriers. Use a shared, secure data platform to track every individual by name, assign a single accountable lead agency per person and monitor progress from first contact through placement in housing or treatment. Treat the pilot as a learning lab — capturing real-time lessons about staffing, legal and policy obstacles; data integration; and cost per successful outcome — to produce by Day 100 a detailed, public plan for scaling citywide, including resource, workforce and policy requirements. The Times Square Alliance is working toward a version of this in West Midtown.
3. Make housing a central piece of the solution
For the unstable, unsheltered homeless population, providing housing without treatment is woefully insufficient, and treatment without housing leaves them vulnerable to a vicious cycle of circumstances that can reverse improvements in their mental health.
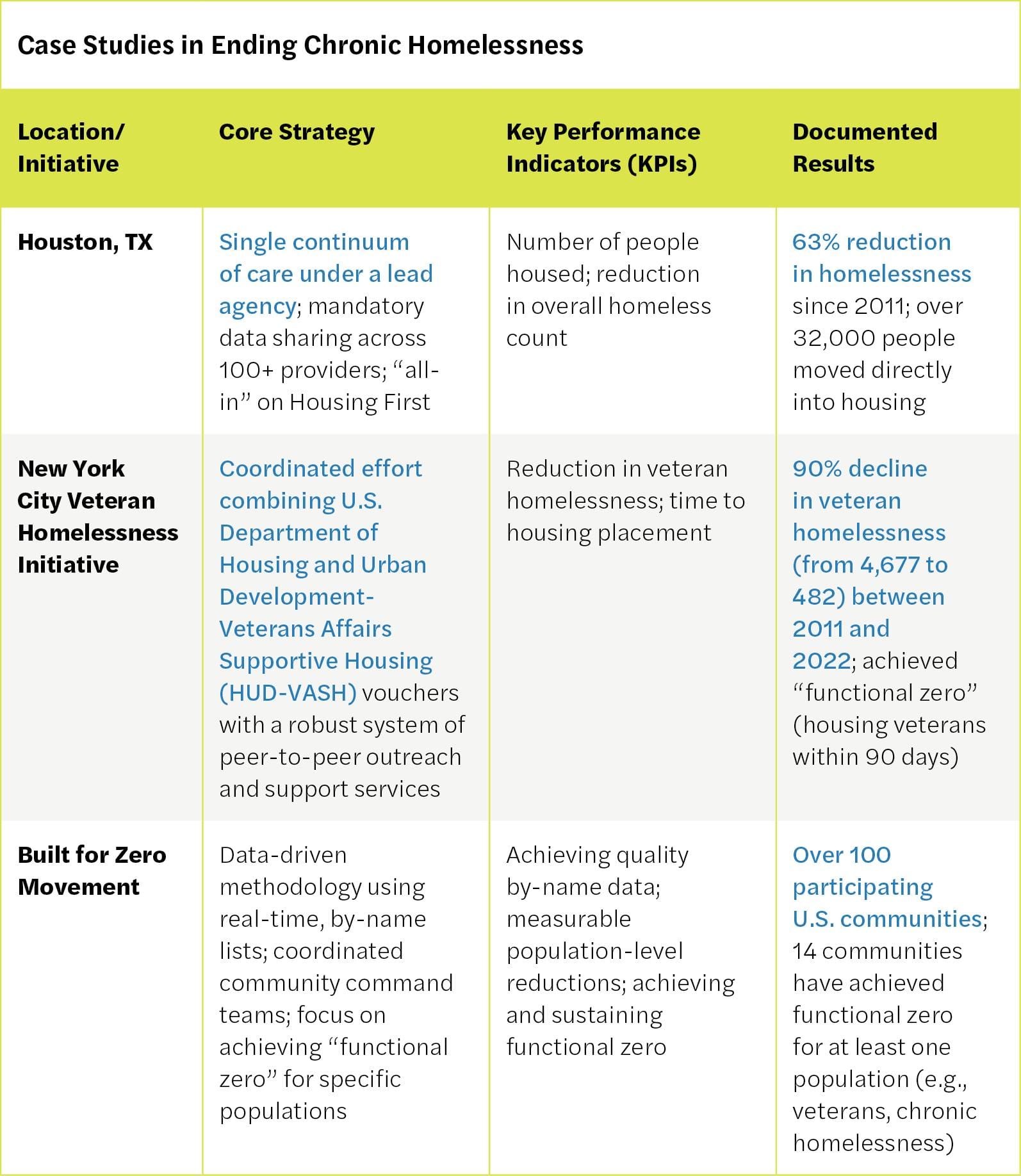
The value of “housing first” has been studied in multiple cities across the nation and the globe. Within the United States, Community Solutions has shown in 15 cities how setting a goal of “functional zero” street homelessness and holding relevant agencies accountable can significantly improve the lives of street homeless people. Evidence from other cities, and New York City’s own past successes, proves its value. Houston moved more than 32,000 homeless people directly into apartments over the last decade, cutting its homelessness by 63%. New York City itself reduced veteran homelessness by nearly 90% since 2011 by rapidly housing every veteran in need.
For people struggling with SMI and related problems, housing must be accompanied with services — meaning it must be supportive. But today, there is a combination of problems: either not enough units, a mismatch between the type of units available and the types of units needed, or bedeviling bureaucratic barriers that keep existing and appropriate units vacant even when there are individuals in need of them. In June 2025, officials reported 5,092 vacant apartments — about 2,200 of which were offline for repairs — prompting new City Council legislation to track vacancies, underscoring that filling existing stock is a fixable management problem. The City’s coordinated entry system is not universally used, so many placements never reach the shared pipeline. The landscape is fragmented across dozens of programs, agencies and categories, leaving specialty beds vacant. On the front end, the application process is slow and paperwork-heavy — creating an especially high hurdle for people living unsheltered.
Specifically, the City should:
- Scale up direct street-to-home placements. The City must immediately expand its successful Street-to-Housing pilot, which moves individuals from welcome centers directly into vacant single-room occupancy units with on-site support staff. The pilot successfully housed 130 people in units that had been sitting vacant for an average of 568 days, proving the model's efficacy and its ability to utilize existing, underused housing stock. This expansion should directly address the paradox of vacant supportive housing units by targeting them for the highest-need population. Whenever possible, individuals should be routed around the shelter system and directly into permanent or semipermanent housing with services. Programs like Volunteers of America's "Street-to-Housing" should be scaled up.
- Streamline eligibility and remove bureaucratic barriers. The City should override, reduce or overcome onerous documentation requirements that delay housing placements. For example, City Council Intro 1100-2024, which would allow time spent incarcerated to count toward chronic homelessness for City-funded housing, should be enacted to overcome the hurdle that current regulations pose to people who would otherwise qualify for housing. The City should simultaneously accept existing clinical evaluations, eliminating redundant paperwork, and devise a single placement packet that follows a person through the process instead of restarting files at every step.
- Expand the supply of supportive housing. The City must continue to increase the number of permanent supportive housing units earmarked for people coming from chronic street homelessness. This includes exploring innovative models that expand housing alternatives including shared housing options and single-room occupancy units with private baths and shared living spaces.
- Establish a real-time "flow desk" and make CAPS the single front door. CAPS is the City's internal database for matching people to supportive housing and other placements. It should serve as the unified entry point for all referrals. Every provider and funder should be required to list vacancies and status updates in CAPS, with automatic escalation for any unit vacant more than 30 days. A public dashboard should display vacancies, number of days vacant and next actions, and future contract compliance should depend on full participation in CAPS. San Francisco's Housing Vacancy Dashboard is a model worth learning from.
- Pay for speed and staying power. The City should link funding to faster lease-up times and require daily vacancy reporting. It should also fund mobile clinical teams to stabilize high-need tenancies and enforce prompt-pay standards so providers can keep units filled.
4. Concentrate outreach, treatment and enforcement on the small group whose instability most endangers themselves or others.
While many unsheltered New Yorkers obey the law, when offenses occur they unsettle the public, making New Yorkers wary of the trains, sidewalks and parks that define public life. Arrests involving this population have risen 38% since 2022. Charges skew toward low-level property and drug offenses, both of which take a toll on our public spaces. Assaults are common as well. Most people are arrested only once. But a small subset is picked up repeatedly and accounts for a disproportionate share of bookings. These incidents concentrate in a limited set of locations, and there is substantial overlap between homelessness, SMI and jail admissions. This suggests the City should triage the small number of individuals and locations that drive most harm. Then it should integrate outreach, treatment, shelter and enforcement in a system designed for repeated contacts rather than one-off interventions. Doing this well requires breaking down data silos across the areas of health, human services and justice so these systems work together rather than at cross-purposes. Specifically, the City should:
- Use routine police encounters to open doors to care. Police are a constant presence in the places where unsheltered New Yorkers live, and it is neither realistic nor desirable to separate them from this work. The City should strengthen existing NYPD-to-DHS referral protocols so that any meaningful contact, even a low-level enforcement like a summons, can trigger a handoff to outreach and care. Referral outcomes should be tracked to ensure these connections are timely, consistent and effective.
- Scale up models proven effective in the most acute cases by building on the symbiotic relationship between IMT and the Step-Down Treatment Ensures Personal Success (STEPS) model.IMT — which deploys multidisciplinary teams that blend public safety with behavioral health — is uniquely effective for the highest-acuity individuals, those with histories of violence and criminal justice involvement. The City should also clear the current waitlist while simultaneously implementing STEPS, a transitional model that allows stable clients to "graduate" from IMT. An evaluation by NYU's McSilver Institute on Poverty shows STEPS’ significant effects in achieving housing stability and avoiding criminal justice involvement while reducing costs and freeing up scarce, high-intensity IMT slots for those currently languishing without care.
- Deploy Forensic Assertive Community Treatment as the default clinical response for the high-frequency / high-harm few. These intensive teams — made up of clinicians, peers and justice-system liaisons — should coordinate closely with outreach workers and, when needed, police. The aim is to ensure that when someone in this highest-need group is encountered, they can move directly from the street into housing with treatment and sustained support.
- Make justice-involved supportive housing (JISH) a far more common discharge pathway from Rikers Island jails for individuals with SMI or repeated homelessness.JISH, a promising model, can enable sharp declines in jail, shelter and crisis-care use, so the City should build on what already works at scale. Officials should use integrated data to trigger more routine JISH referrals before release and reserve units for those cycling through jail, hospitals and the streets. It should hold DOHMH, H+H and the Mayor's Office of Criminal Justice jointly accountable for placements, housing retention and reductions in jail readmissions.
- Use involuntary removals strategically for the small subset of people at clear and imminent risk. The City should ensure each involuntary removal is tied to a clear stabilization plan, with a bed and clinical follow-up arranged prior to discharge. It should treat police, hospital and court encounters as opportunities to interrupt dangerous deterioration, not as routine returns to the street.
5. Escalate outreach and use involuntary removals strategically
For individuals who present a danger to themselves or others who will not accept help voluntarily, the City needs to employ involuntary mechanisms in a way that improves results for the people affected, instead of cycling them through shelter, hospital and jail. The goal must be removal with treatment and housing. The law permits involuntary transport to a hospital when a person is a danger to themselves or others, a definition of danger that includes one’s inability to care for their own basic needs. It further allows an individual to be held for treatment if they continue to meet the statutory criteria for involuntary admission. Both authorities should be used more fully and assertively for those who repeatedly cycle through crises. At the same time, every instance of involuntary transport or commitment should be viewed not as an end, but as the beginning of a sustained intervention. Specifically, the City should:
- Improve the productivity of street outreach and clinical capacity, and assess where police are a necessary part of the process. The City should first assess whether there are enough outreach teams with the kinds of skills that can connect people in need to stable housing. The relevant data to assess capacity are not currently public. But discussions with nonprofits and government strongly suggest the need for a more organized, person-oriented and sustained approach. Alongside this assessment, the City should determine what mix of skills — from clinicians to social workers to police — is required.
- Empower more responders to initiate emergency removals. Practically and legally, police are needed to effect most removals where a person is believed to be a danger to themselves or others. To increase timely intervention, the State should consider learning from Durham, North Carolina, and expand the authority to involuntarily transport someone to other trained professionals such as paramedics or outreach-team supervisors. This would reduce delays and overreliance on police, who don't always have the clinical training to know what they are seeing.
- Pair involuntary removal with continuous outreach and placement support. When someone is taken involuntarily to a hospital, an assigned outreach team should remain responsible through treatment, discharge and housing placement. The protocol should automatically alert housing and care coordinators at admission so planning begins on Day One. Each involuntary intervention must trigger a full-cycle response, ensuring that every person enters a sustained pipeline of treatment, housing and follow-up rather than cycling back to the street.
- Track and evaluate outcomes of involuntary interventions. Because coercive measures demand heightened scrutiny, the City should rigorously monitor what happens after involuntary removal or court-ordered treatment, tracking outcomes such as housing stability, ER visits and arrests to assess effectiveness and refine the approach.
- Build comprehensive case files for hospital referrals. The City should ensure that when people are brought to hospitals through involuntary removal or referral, clinicians receive a full history of prior contacts, interventions and risks. Equipping doctors with this context enables better-informed decisions and reduces the risk of revolving-door discharges.
- Reform Assisted Outpatient Treatment (AOT) to broaden its impact. AOT under Kendra's Law can be a powerful tool, but it should be modernized to reach more people. This includes tailoring it for diagnoses beyond schizophrenia / bipolar disorder, expanding mental health professionals who can be involved in court decisions beyond physicians (e.g., psychiatric nurses) and integrating it with priority housing placements (a proposal the governor has advanced).
6. Reform contracting and rationalize the budget
New York spends heavily on responding to SMI and homelessness — an estimated $4.6 billion of the City’s budget, with the vast majority of that spending going to operate the city’s massive shelter network, where some 90,000 people sleep on any given night. However, the problem is complicated by fragmented funding sources and siloed agencies. The City cannot tell how much it spends on a single individual as they cycle through the streets, programs, hospitals, jail and shelter because funding is tracked by service, not by person or outcome.
This fragmentation obscures critical trade-offs. A City comptroller report on Housing First strategies laid bare the challenge: Supportive housing costs $68 per day per person versus $1,414 for jail or $3,609 for hospitalization. Yet agencies continue to fund expensive emergency responses because they cannot see the full picture. Simultaneously, contracts reward activity over outcomes, and chronic payment delays force nonprofits to float City services.
Rationalizing the budget means buying results, paying providers on time and publishing an honest, multiyear price tag for the full plan. It means investing in housing and clinical care today to avoid ER and jail costs tomorrow.
The City is not starting from scratch. HPD’s fiscal year 2026 capital plan calls for committing $12 billion in City subsidies for affordable housing over the next four years, including at least $1.8 billion for supportive and special needs housing. That is enough to build more than 10,000 supportive units — sufficient to house every unsheltered New Yorker. Additionally, social service agencies will spend nearly $8 billion in fiscal year 2026 on homeless shelters, rental assistance, public assistance, mental health programs, and substance abuse initiatives. Much of this agenda could be paid for simply by spending these billions more effectively to stem the inflow of people into shelter.
This efficiency extends to operations. The City and State already support multiple different kinds of outreach and response teams. Whether deploying city workers or nonprofit employees, utilizing civilians is generally less expensive than funding police officers. The cost effectiveness of this response depends on the City’s ability to steel itself to figure out what works for whom, and deploying those teams accordingly.
New York is not exceptional. Eugene, Denver, and Houston addressed their homelessness problems with fewer resources and smaller tax bases. According to the Lincoln Land Institute’s Fiscally Standardized Cities database, New York City collected 20% more total revenue per capita in 2022 than Denver, twice as much as Houston, and 1.7 times more than Eugene. While legitimate differences exist — those cities have lower housing costs and no right to shelter — we have the means.
To coordinate and rationalize the city’s spending on troubled unhoused people, the City should:
- Perform an initial, rapid assessment of the degree of need for additional staffing — and of what kind — for outreach and response. This assessment is the first step towards synthesizing the multiple different approaches from the city, the state and nonprofits and assessing what additional resources, if any, are needed. With many of the outreach and response responsibilities possibly moving over to the new proposed Department of Community Safety, this is an irreducible minimum necessary step.
- Perform a citywide assessment of the number of potential sites for supportive housing and the allocated budget amounts. Another irreducible minimum necessary step towards solving the issue of those living with serious mental illness on the street.
- Reassess and renegotiate contracts to buy better outcomes, not volume. The City should rebid or amend agreements to align incentives with results.
- Pay providers on time and at full, transparent cost. Late payments are a major challenge to nonprofit operations. The City should set a strict prompt-pay standard with automatic interest, provide mobilization advances on new contracts, adopt standardized indirect/overhead rates and inflation indexing, and clear existing invoice backlogs via a centralized portal.
- Consolidate fragmented funding into unified budget lines with transparent allocations. The City should create a single SMI/homelessness budget dashboard that systematically tags and tracks federal, State, City and philanthropic dollars by provider, program and outcome. This would enable the City to follow funding more clearly — across DOHMH, DHS, H+H, NYPD, FDNY, the Department of Correction and other agencies — and enhance accountability.
- Implement cross-agency individual tracking and outcome-based funding that follows the person, not the program. To rationalize budgeting, the City should assign each individual a unique identifier across all agencies and providers to track their complete service journey and total cost. It should then pilot bundled payment models where a lead provider receives a single allocation to coordinate all services for high-utilizers — housing, clinical care, crisis response — with payment tied to stabilization outcomes (days housed, hospitalizations avoided, jail stays prevented).
7. Follow the evidence
Ultimately, neither crisis nor ideology should guide New York City’s approach to dealing with the challenges of this population; results should. To that end, the City should approach these solutions with a measure of humility and demand rigorous and independent evaluations of all of its programs so that it can adapt strategies at multiple steps along the way. The next mayor should cut strategies that fail to yield results and redouble investments as soon as solid evidence of their success emerges. To do this, the City should:
- Create a fast-track pathway for evidence-based innovations. Establish a mechanism for piloting and scaling new approaches without waiting years for full request-for-proposal (RFP) cycles. Set aside flexible funding and preapproved contracting pathways that allow successful pilots to shift quickly into ongoing programs.
- Identify and align key outcome metrics. City Hall should standardize outcome metrics across systems to determine whether initiatives should continue, expand or end. This should include metrics that capture the connection or lack of connection to different programs across the system (e.g., from outreach to treatment placement). All service providers and government agencies should be onboarded and trained on their responsibilities and expectations for how they will engage with data collection and reporting.
- Develop an evaluation framework that is aligned with system response. The City should adopt a standardized evaluation framework tailored to each stage of the system, allowing for meaningful comparisons across providers and models. The City should support mixed-method evaluation designs to capture a broad set of outcomes. Findings should feed directly into program and funding decisions.
- Prioritize evaluations for programs with no rigorous evaluation. Expanded programs that have never undergone independent evaluation should be first in line for analysis. Evaluators should be allowed to choose the most appropriate methods — qualitative, quantitative or hybrid — to assess impact.
- Ensure accountability mechanisms in contracting to continue or stop programs. City contracts should include clauses requiring programs to continue, expand or end based strictly on evaluation results.
What not to do
DON’T abandon supportive housing or Housing First programs.Decades of research show housing is highly effective.
DON’T remove police from the equation, but balance their use. Some situations involve genuine threats where only trained police officers can ensure safety. The key is a balanced deployment where police serve in a supporting role when necessary, and their routine contacts with people in need for a wide range of reasons can serve as vital linkages to care.
AVOID using criminal law as a pretext or default means for managing illness-related behavior. Arresting people for minor infractions that stem from mental illness is a temporary fix for the general public and is usually counterproductive for the person with an illness. Enforcement should focus on serious or dangerous conduct and on repeated refusals to stop unlawful behavior, not on the behavioral symptoms of a person’s illness or low-level acts that pose no real threat.
DON’T conduct encampment sweeps without offering services and housing. Clearing a homeless encampment without providing a better alternative is a local, temporary measure that displaces the problem. Any cleanup must be paired with intensive outreach and transportation to a waiting bed.
DON’T shuffle people between systems without continuity. Every transition — from jail to community, hospital to shelter — should be purposeful and managed with seamless handoffs and continuous case management to break the cycle of people falling through the cracks.
DON’T treat all cases the same. Homeless individuals with SMI have a range of complex problems that require different responses. Interventions should be tailored to the individual, using the full range of available tools rather than a single uniform response.
DON’T create or expand programs when evidence is lacking. Pouring more money into fragmented or unproven efforts will not yield results. Growth must be strategic and coordinated, aimed at creating a leaner, smarter system, not just a bigger one. Providers and City officials should partner with independent researchers to evaluate not just services delivered but actual improvements in health, safety and quality of life.
Advisors
We are grateful to a core group of people listed below who generously gave their time and wisdom, meeting as a group and individually, in writing and in conversation, as Vital City worked through these recommendations. We are particularly grateful to the many talented writers, researchers and doers who helped produce these recommendations, including Allie Meizlish, Archana Jayaram, Tamiru Mammo and Gail Nayowith.
The recommendations are Vital City’s and do not necessarily reflect the positions of any person or institution listed below. Any errors are our own.
ALEX CROHN, deputy commissioner of strategic initiatives, NYPD
DENNIS CULHANE, University of Pennsylvania
BRANDON DEL POZO, Brown University
LINDA GIBBS, Bloomberg Associates; former NYC deputy mayor for health and human services
DAVID GREENBERG, CFO, Vibrant Emotional Health; former deputy director, NYC Mayor’s Office of Management and Budget
JOHN HALL, NYPD / MTA Police Department (ret.)
HILLARY KUNINS, former executive deputy commissioner, NYC Department of Health and Mental Hygiene
JONATHAN McCLEAN, CEO, CASES
MEG REISS, Chief Assistant District Attorney, New York County
CHERYL ROBERTS, executive director, Greenburger Center for Justice
BRENDA ROSEN, CEO, Breaking Ground
JODY RUDIN, CEO, Institute for Community Living
BRIAN STETTIN, senior advisor on severe mental illness, NYC Office of the Mayor
TERRI TOBIN, Chief Advisor, NY/NJ HIDTA.
ANNE WILLIAMS-ISOM, former NYC deputy mayor for health and human services
There are many other people in the New York State and New York City governments as well as in the numerous nonprofits who work tirelessly on this issue and who shared their knowledge of how things actually work, not just as they appear on paper. A partial list of the agencies and offices include: the New York City Mayor’s Office, the Office of the Comptroller of New York City, the New York CIty Police Department, the New York City Department of Health and Mental Hygiene, the New York City Department of Homeless Services, Fountain House, Times Square Alliance, among others. We are deeply grateful for their time and advice, and for their service to the people of New York City.
════════════════════════════════════════
New York is entering an historic and pivotal transition. Mayor-elect Mamdani faces big problems on housing, safety, mental health, transit, and more.
Vital City is uniquely positioned to offer clear, practical guidance rooted in evidence. Ideas that could actually be implemented and work.
But to meet this moment, we need to grow.
That’s why, this year, for the first time, we’re asking our readers to support Vital City directly. We’re aiming for 700 inaugural supporters by December 31.
Your support will help us expand our editorial capacity, strengthen our operational support, and continue delivering thoughtful, relevant and informative work in 2026.
If this article informed your thinking, challenged you, or helped you understand the city more clearly, please consider supporting the work behind it.
Make your tax-deductible gift and help us reach 700 supporters.
Vital City



