
This is one of three supporting documents connected to Vital City’s recommendations on serious mental illness and homelessness,
A profile of the population
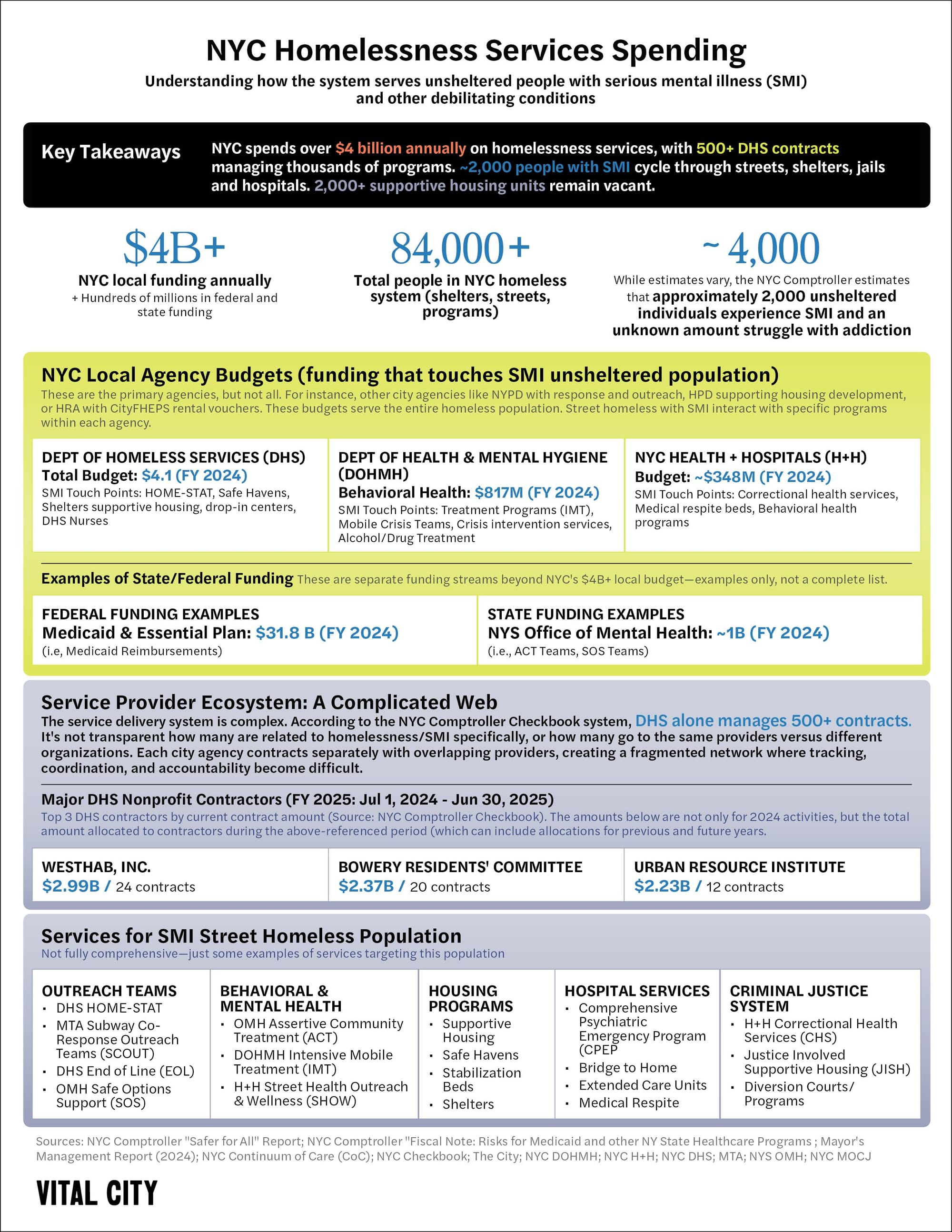
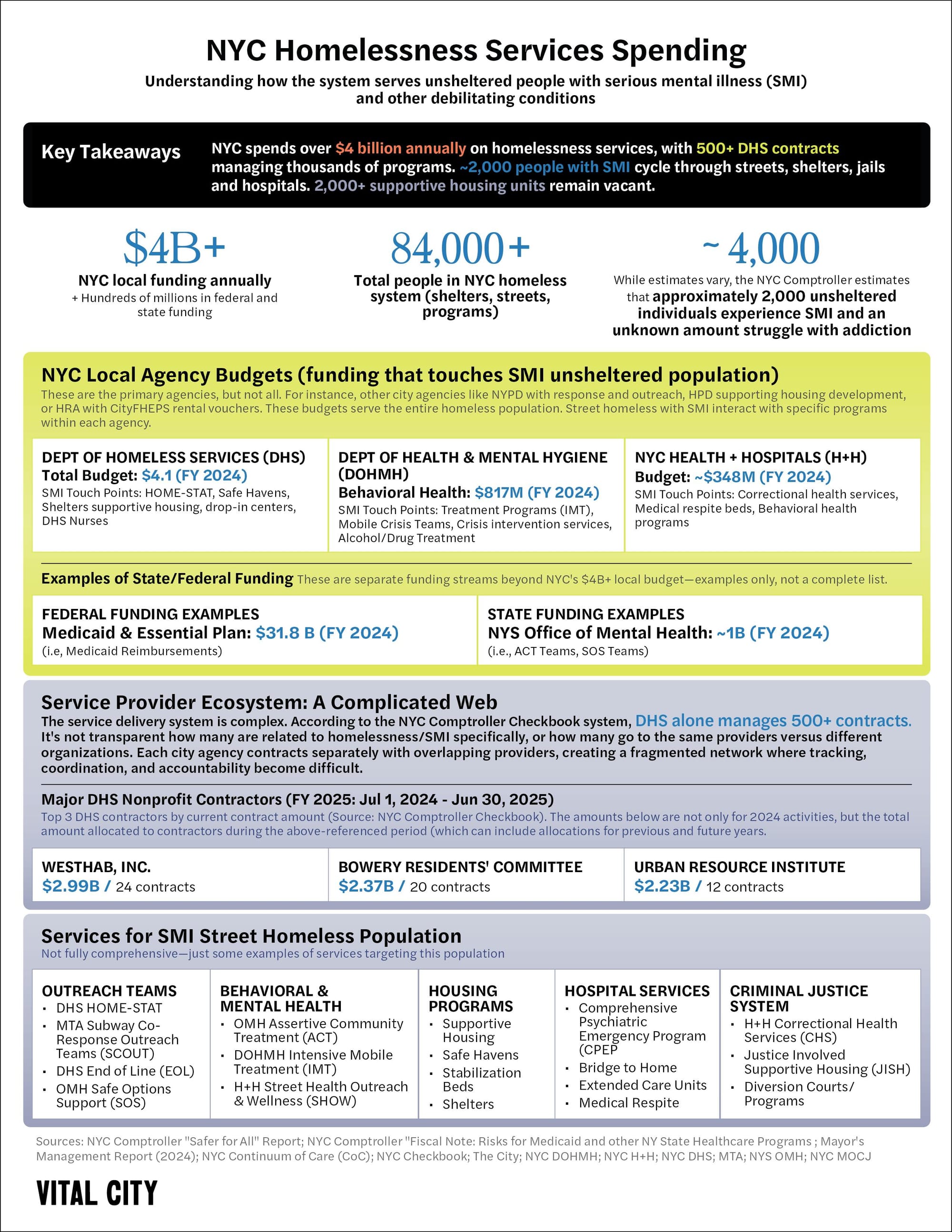
On any given night, about 4,000 people are living on the street in New York City. That figure, drawn from a point-in-time count, understates the scale of the problem: Because people cycle in and out of unsheltered homelessness, the number of unique individuals affected over the course of a year is likely much higher.
New York isn’t alone among American cities in facing this issue: In fact, the scale of the problem is not especially bad by some measures. Unlike most large U.S. cities, which have larger unsheltered populations as a portion of all homeless individuals, New York guarantees a temporary bed to anyone who needs one. This legal right to shelter and the network of facilities that go with it keep roughly 95% of homeless people indoors, leaving a concentrated group with acute needs and a demonstrated reluctance to accept a shelter bed (or sometimes even a nonshelter bed) on the street. In a dense city, the visibility of this troubled population can fuel perceptions of disorder and personal risk that exceed the problem’s actual scale.
Within this population, needs and circumstances vary widely. Many people grapple with serious mental illness and/or substance use disorders. Some have conditions such as schizophrenia or bipolar disorder that respond to sustained treatment and support; others live with personality disorders that require long-term psychosocial care. Co-occurring substance use is common and complicates engagement; to the untrained eye, a seeming mental illness crisis may in fact be drug-induced psychosis that wears off when the drug’s effects subside. Another complicating factor is traumatic brain injuries (TBI), which is estimated to affect more than half of people experiencing homelessness.
While it’s true that a person who is homeless is more likely to be a victim than a perpetrator, unstable people living on the street can indeed pose serious safety risks. In 2024, 1,285 street-homeless people were arrested for assault, a rate more than 20 times that of the total city population. Yet criminal offending isn’t a factor in prioritizing who gets the most focused attention, even on the City’s “Top 50” lists — the informal name for the internal rosters used to coordinate work on the most serious subway and street cases.
Particular crimes committed by these individuals loom large and heighten public fear. There was the fatal 2022 subway shoving of Michelle Go in the Times Square-42nd Street station and, more recently, the 2024 stabbing spree across Manhattan that left three people dead. Untreated illness and addiction also often manifest as erratic behavior that many experience as threatening. For the individuals themselves, surviving in public without effective care means worsening health, criminal justice involvement, vulnerability to victimization and repeated emergencies, often resulting in an unbroken cycle through the street, shelter, ER and jail akin to those Dr. Ross MacDonald identified in his analysis of Rikers Island “hot spotters.”
What government currently does about the challenge
Billions of public dollars are spent each year on both homelessness and behavioral health, yet this specific cohort remains too disconnected from sustained attention, typically cycling through brief and redundant contacts with police, hospitals and shelters before returning to the street. The visible churn convinces the public that government cannot care for the most vulnerable people or maintain order in common spaces.
Of course, even if everything ran like clockwork, there would be crises and failures. These are bedevilingly difficult cases to manage. Government and nonprofit providers put an enormous amount of thought and commitment into addressing difficult circumstances. But far too much effort, money and time are squandered because multiple systems operate in parallel — the police, 911 and 311, EMS, homeless-services outreach teams, public hospitals and nonprofit providers. Each has different mandates, funding sources, data systems and protocols. Handoffs are inconsistent; information is siloed; continuous case management and accountability are absent. Outreach teams often lose track of clients once cases move outside their geography or specialty. Hospitals frequently discharge psychiatric patients back to the street after brief observation because longer-stay treatment beds and step-down options are scarce. Judges who see mentally ill or drug-addicted defendants have few viable pathways to secure treatment instead of jail because effective programs have limited slots. At Rikers Island, an estimated one-third of people admitted in 2023 were homeless before arrest; upon release, only about 3% of detainees with serious mental illness were connected to supportive housing, with most returning to shelters or the street.
1. Contact with individuals in crisis and what follows
It’s not easy to get one’s arms around all the opportunities for official intervention — the many ways in which a seriously mentally ill or otherwise unstable homeless person living on the street encounters police, mental health professionals, social workers and others — but it’s important to try to see the current tangled system in all its complexity.
There are two primary ways unsheltered individuals in public spaces with serious mental illness will make contact with the system: police dispatch (i.e., 911) in response to a crisis, and outreach teams (sometimes civilian, sometimes a mix of police and civilian) that initiate contact with individuals even when there is no reported emergency.
After an encounter, police (usually) can transport an individual involuntarily to a hospital for a psychiatric assessment if they’re in psychiatric distress and qualify for transport, which under the law is defined as presenting a danger to themselves or others, a definition that includes the inability to take care of their own basic needs. If the person does not qualify for involuntary transport, then they could either be arrested if alleged to engage in criminal activity, or offered to be connected to different services (e.g., housing).
Not all people who live on the street are in the throes of crisis, but crises happen with some level of frequency. New York City’s behavioral health crisis response still defaults to 911, with police and EMS as the primary responders. The NYPD fields more than 150,000 calls each year involving psychiatric distress (a number that includes people who are housed). Police are usually present for three reasons: the possibility of violence, social workers’ preference for backup in unpredictable situations and the legal requirement that only police can carry out involuntary transports.
Alongside 911, 311 serves as the City’s nonemergency intake and routing line for homeless-related concerns. In 2024, the DHS (Department of Homeless Services) handled about two-thirds of these calls, and the NYPD handled the remaining third. Among the City’s outreach efforts, co-response teams — the MTA’s clinician-led SCOUT (Subway Co-Response Outreach Teams), a daytime program conducted in partnership with DHS, and PATH (Partnership Assistance for Transit Homelessness), an overnight program led by the NYPD, DHS and the City’s public hospital system — are among the most recently conceived initiatives. These teams work to actively find and engage people in distress instead of waiting for a call to come in. Their models pair mental health clinicians with police officers to handle crises together, combining treatment expertise with public safety backup. (Though they are expanding, they remain small: SCOUT began with two pilot teams and is slated to reach roughly 10 by year’s end. PATH does not publish similar numbers.)
There is growing interest, including by Mayor-elect Mamdani, in the City’s B-HEARD (Behavioral Health Emergency Assistance Response Division) pilot — unarmed teams of clinicians and EMTs dispatched to eligible mental health 911 calls instead of police — as an alternative. The program’s current footprint in 31 precincts (of 78) and roughly 15,000 calls handled in 2024 remains a small amount relative to need. And, as with many if not all of the programs and approaches, there has been no reliable (or publicly available) assessment of what kinds of problems B-HEARD is effective at addressing and what it is not.
B-HEARD was modeled on CAHOOTS in Eugene, Oregon, pairing health professionals with responders for behavioral health crises, but it does not fulfill the same role. CAHOOTS (Crisis Assistance Helping Out On The Streets) combines crisis response with sustained, proactive outreach in the community, while in New York City that outreach is handled by separate street outreach teams rather than B-HEARD. B-HEARD focuses on reacting to selected 911 calls during limited hours instead of serving as a default, community-based alternative. The result is often trading one type of responder for another rather than changing how and when help reaches people.
Both strategies, B-HEARD and involuntary transports, suffer from an absence of sufficient publicly reported outcome measures to tell policymakers whether these responses actually improve stability, reduce repeat crises and connect people to care. This makes it difficult to evaluate their effects and determine whether they’re as effective as other nonpolice alternative response programs (e.g., Denver’s STAR (Support Team Assisted Response)).
This raises a crucial recurring theme: The orientation of the current system — to deal mainly with point-in-time crises instead of sustained attention to a particular person throughout their life course — means that neither government nor anyone else with responsibility has a panoramic view of how any one individual is doing after the crisis.
Much of the public reporting on these efforts remains focused on activity — contacts, referrals and transports. But there is little known about durable results such as housing retention, reduced crisis recurrence or diversion from the justice system. Without those measures, it is difficult to know whether scaling up is translating into lasting impact.
By contrast, several civilian outreach models have expanded in recent years. State OMH’s (Office of Mental Health’s) SOS (Safe Options Support) teams grew from four to 20 between 2022 and 2025, with press coverage citing State data showing 800 people placed into permanent housing in New York City from April 2022 to April 2025 after 58,000 engagements. SOS teams are multidisciplinary groups (clinicians, peers and care managers) who do persistent, field-based outreach both topside and underground, stay with people to help navigate paperwork and appointments, and broker placements into Safe Haven / stabilization beds and supportive or permanent housing.
The City has made numerous concerted efforts to knit together the fragmented system and focus on those in greatest need. One example is the StreetSmart application. StreetSmart, a project of the Department of Homeless Services, is a digital by-name list — a shared, person-specific roster used by City-contracted outreach providers to track individuals living unsheltered and to record engagements and progress over time. This is a real innovation. Unfortunately, it excludes many nonprofits that are not under City contract and therefore are not bound by the City’s privacy rules. Health, housing and police data are not integrated, and health-privacy rules restrict certain types of data sharing. These gaps make it difficult to measure outcomes or coordinate care effectively.
2. Involuntary Transport & Hospitalization
After a response or outreach team makes contact with an unsheltered individual, the next step is assessing whether the individual is in psychiatric distress. If an individual is in crisis, both police and clinicians have the power of involuntary removal to a hospital (under New York State Mental Hygiene Law Sections 9.41 and 9.58). The current administration has leaned into involuntary transport to hospitals under the Mental Hygiene Law as part of its strategy. It’s unclear whether expanded use of involuntary transport will break existing cycles or worsen them — an uncertainty the City should resolve through rigorous evaluation. It is critical that the City learn what the results are so that it can determine how most effectively to implement the law. In 2024, police initiated about 7,000 involuntary transports (Section 9.41), roughly two-thirds of which originated from 911 calls. Clinicians accounted for another 661 (Section 9.58). There is no public accounting of whether the removals in 2024 are more or fewer than in the past. Also, while 57% of individuals transported pursuant to an order issued by a clinician (9.58) are admitted, there is no public reporting on how many individuals are admitted into psychiatric care after a police transport (9.41).
Once at the hospital, a person can be held for a short evaluation under Section 9.40, typically lasting up to 72 hours. This evaluation typically occurs in a CPEP (Comprehensive Psychiatric Emergency Program) unit, the designated psychiatric emergency department. If doctors determine that the person still needs inpatient care, they may be admitted under Section 9.39, which allows up to 15 days of emergency hospitalization. For people who continue to need treatment, the hospital can extend the stay under Sections 9.27 or 9.37, based on certification by doctors and a psychiatrist, for up to 60 days. If more time is required, the hospital must seek a court order under Section 9.33 to keep the person longer. A small number of extended-care units provide about 90 to 120 days of treatment, and there are also medical respite beds for patients with physical health needs.
If an individual is not admitted or discharged, options are extremely limited. Even if admitted to psychiatric care, individuals may face prolonged waits in emergency departments due to psychiatric boarding — when patients remain in the ER for extended periods because no inpatient psychiatric beds are available. There are few alternatives for those not admitted and difficulty accessing long-term or supportive housing options to ensure stability after discharge.
It is also worth noting that some constraints concerning long-term psychiatric care stem from State and federal financing and regulatory rules that limit what care is available and for how long, notably Medicaid’s IMD exclusion, which generally prevents federal funding for adults aged 21 to 64 receiving care in psychiatric facilities with more than 16 beds.
3. Treatment and other services
While improving the initial response to individuals in crisis is often presented as central to solving the problem, changing who initially responds when a crisis happens is not enough. If an individual is not admitted to a hospital or arrested, what happens next is typically what matters most. Same-day clinical access? Intensive Mobile Treatment (IMT), which provides support and treatment in streets, shelters and public spaces? Detox and step-down care? Supportive housing with services? And is there a smooth transition to this help?
Without the right resources at the right moment, most encounters eventually result in the person cycling back to emergency rooms, shelters or the street. B-HEARD can reduce police call volume, and it might reduce the risk of a given incident escalating, but it does not address the underlying problem of “What next?” or necessarily address the underlying problem motivating the report.
Again, the “What next?” question rears its head. The City does not publish systemwide data on how many of the police-initiated transports result in admission or for how long or what happened to the person upon release.
Treatment following inpatient hospitalization is crucial. Assisted Outpatient Treatment, which is court-ordered under Kendra’s Law, gives individuals psychiatric treatment plans to follow once they’ve been stabilized. It is an important piece of the puzzle, especially given evaluations both within and outside of New York that have found it to be effective in reducing psychiatric episodes and improved outcomes.
OMH’s Assertive Community Treatment (ACT) shows promising evidence of stabilizing housing and reducing psychiatric crises. ACT serves adults with the highest, ongoing psychiatric needs; multidisciplinary teams provide community-based care with small caseloads, 24/7 crisis coverage and time-unlimited support for as long as the person benefits. Similar to ACT, the Mayor’s Office of Community Mental Health has implemented IMT teams that serve adults with serious mental illness who are often street- or shelter-based, recently incarcerated or repeatedly hospitalized. IMTs meet people in the field at points of crisis or transition (street, ER or jail/prison discharge) and remain engaged as long as clinically needed, often many months, until a step-down is appropriate. For IMT, however, a 2024 City comptroller audit found issues with tracking outcomes and program management. Incarceration data were not regularly tracked and treatment engagement was inconsistently measured. Reviews of providers varied in quality, follow-up on corrective actions lagged and the program still lacks transparent, system-level reporting to demonstrate durable outcomes — a gap also highlighted by a New York Times investigation into the City’s fragmented mental health response. However, mobile treatment capacity is constrained: The City funds 31 IMT teams serving fewer than 1,000 clients, with similar pressure on State-funded ACT teams.
It is also worth noting that some constraints concerning long-term psychiatric care stem from State and federal financing and regulatory rules that limit what care is available and for how long, notably Medicaid’s IMD exclusion, which generally prevents federal funding for adults aged 21 to 64 receiving care in psychiatric facilities with more than 16 beds.
4. Shelter and housing placements
Housing must be a central part of the approach to stabilizing people who lack it and are on the verge of psychiatric crisis. But even when the City can identify and reach people with the highest needs, individuals are typically routed to places that are, by design, temporary, including ERs; crisis respite centers; Safe Havens, which are low-barrier, small-scale programs that provide private rooms and flexible rules for people coming directly from the street, who often resist traditional shelters due to their safety records, strict curfews, sobriety requirements and other rules; stabilization beds, which are low-threshold beds for a high-functioning population; general shelters; or short jail stays.
Some of these placement failures could be addressed by increasing Safe Haven and stabilization beds, speeding documentation, expanding mobile treatment capacity and improving handoffs.
Supportive housing — permanent affordable apartments with on-site services — is by far the most crucial component of any system to help this population. Yet today, approvals do not reliably translate into placements for unsheltered individuals. Despite the strong evidence base concerning the effectiveness of supportive-housing programs, outreach programs have struggled to secure housing placements. In 2024, outreach teams secured supportive-housing approvals for 955 unsheltered people, but only 175 (18%) obtained a unit, often due to process barriers; at the same time, more than 4,100 supportive-housing units sat vacant. Unsheltered homeless people don’t just suffer from mental illness and addiction; they lack, and need, some community. Here, clubhouses like those run by Fountain House have helpfully expanded in recent years, giving individuals a psychologically healthy place to go during the day and a connection with related services. A person who is connected with others is more likely to get the help they need when they need it.
5. Criminal justice interactions and what follow
In some instances, the initial interaction with police stems from criminal behavior. In 2024, NYPD recorded 15,274 arrests of unsheltered New Yorkers. Most commonly, these arrests are for petit larceny, misdemeanor drug offenses or assault charges.
When a police officer makes an arrest, the defendant is charged and brought before a judge for arraignment. At arraignment, the judge has the option to release the individual on their own recognizance pending the resolution of the case, release with certain conditions or set bail and hold the individual in detention. In the case of homeless individuals, lack of stable housing is sometimes considered by judges in determining risk of flight, and any amount of bail could effectively result in being held in jail pending trial if they are unable to afford it.
For individuals who appear to have a serious mental illness, judges will sometimes order an exam under Criminal Procedure Law 730 (”730 exam”), to determine whether the individual is an incapacitated person — a defendant who “as a result of mental disease or defect lacks capacity to understand the proceedings against him or to assist in his own defense.” For underlying misdemeanor charges, a finding of incapacitation results in the dismissal of the underlying misdemeanor case as well as care and treatment in an appropriate institution for up to 90 days. For felony cases, longer orders of commitment are possible, and the status of the underlying criminal case will depend on whether or not it is ultimately indicted by the prosecutor. In cases of an indicted felony, the individual can be held in a State forensic psychiatric facility for up to two-thirds of the maximum sentence if the patient had been found guilty of the underlying felony. It is also worth noting that the process of 730 exams can often lead to many case delays and a much lengthier stay of incarceration or time in a psychiatric facility for individuals with serious mental illness.
In the absence of a 730 exam, prosecutors still have many tools at their disposal for individuals living with serious mental illness and/or substance use disorder. Included in these options are mental health and drug-treatment courts, as well as the possibility for treatment as a condition of a plea deal or as part of a final sentence.
For those who are living with serious mental illness who are held in jail, there are specialized units called CAPS (Clinical Alternative to Punitive Segregation) units, as well as therapeutic beds, which provide treatment for individuals with serious mental illness while incarcerated. If convicted of a crime and transferred to State custody, there is a continuum of care for incarcerated individuals offered by OMH, including the Central New York Psychiatric Center as well a statewide network of clinics, crisis beds and intermediate care program beds.
Upon release, reentry services are available through nonprofits, NYC Health + Hospitals programs and other City programs, such as the Community Justice Reentry Network, that provide a variety of connections to treatment, care, housing and employment resources.
These are hard cases. Providing services to people living with mental illness is much more complex than providing food to the hungry. Many people of greatest concern do not realize they are ill, a condition known as anosognosia. Others carry trauma or deep distrust of systems and may refuse help repeatedly. Even a well-functioning system is likely to fail more often than it succeeds. But today, batting averages are dangerously low. The system’s flaws are clear: Information is siloed, coordination across agencies is thin, services are poorly matched to need and unevenly distributed, connections are not sustained as symptoms change over time and there is little culture of disciplined self-assessment or course correction. As with every other aspect of engagement with those living with serious mental illness and/or homelessness, the description of the system process does not always align perfectly with delivery. Often there are not enough services, treatment programs, beds or housing options to meet the needs of the individuals these were created to help.
Appendices
NYC homelessness & mental health budget (2024)
| Agency | Line Items | Amounts (2024) |
|---|---|---|
| DHS | Outreach, Drop-In, Reception | $303.7M |
| DHS | Family Shelter Operations, Intake, Administration | $1.1B |
| DHS | Adult Shelter Operations, Intake, Administration | $969.16M |
| DOHMH | Mental Health Services | $601.56M |
| DOHMH | Alcohol and Drug Prevention, Care and Treatment | $153M |
| DOHMH | Developmental Disabilities | $10M |
| DOHMH | Administration | $52M |
| H+H | Correctional Health Services | $285M |
| H+H | B-HEARD | $13M |
| H+H | Mental Health Service Corps | $12M |
| H+H | Just Home | $1M |
| H+H | DOHMH (Transfer) | $37M |
| FDNY | B-HEARD | - |
| FDNY | Emergency Medical Services | $427M |
| OTI/311 | 311 | $61M |
| OTI/311 | 911 | $101M |
| OTI/311 | Administration, Operations | $66M |
| NYPD | Transit | $291M |
| NYPD | Training | $136M |
| TOTAL | $4.62B | |
| TOTAL | $10.4B | |
The evidence backing various policy approaches
The evidence table below does not attempt to rate the level of evidence for the programs indicated. Instead, it aims to be illustrative and provide an overview of what data and research are available for the programs.
NYC programs: evidence and evaluation
| Category | Program Name | Description | Size and Stats | Evaluation |
|---|---|---|---|---|
| Crisis Response and First Response Programs | ||||
| B-HEARD | Behavioral Health Emergency Assistance Response Division: health and mental health-only response to 911 calls; operated by FDNY EMS and H+H | 33,000 responses citywide (2024) | NYC Evaluation City Council evaluation found 88% of calls were resolved without police, EMS or hospital transport, with higher success in non-housing conditions. | |
| Subway Safety (Subway Safety Unit) | Operation to clear the subway of homeless people, involving NYPD and social workers (initially a temporary NYPD pilot); homeless people relocated to shelters and/or hospitalized; program has been the subject of legal challenges | 1800 outreaches 1150 subway removals (2024-to-date) | NYC Evaluation No city evaluation has been performed; advocacy groups have raised concerns about quality of outreach. | |
| Directive 25 (NYPD Directive 25) | Directed "street homeless" individuals with mental illness to be involuntarily hospitalized. | Unknown citywide At least 2000 interactions (2023-to-date) | NYC Evaluation No city evaluation has been performed; advocacy groups have raised concerns about implementation quality and protections against involuntary care. | |
| MCTs (Mobile Crisis Teams) | Nonpolice mental health response for individuals in crisis; may be accessed via 311/988 | 200,000 responses citywide (2023) | NYC Evaluation An evaluation of a different city effort resulted in reductions of arrests, psychiatric hospitalizations and emergency room visits. | |
| CPEPs (Comprehensive Psychiatric Emergency Programs) | State-regulated 24/7 psychiatric emergency programs; recent State capital expansion initiative | 11 programs through H+H (2024), additional programs through private hospitals | No NYC Evaluation An evaluation of a similar program in the Midwestfinds effective results. | |
| AOT (Assisted Outpatient Treatment) | Court-ordered outpatient treatment administered via OMH/localities | 47,000 investigations, 96% petitions granted | NYCa href="https://static.prisonpolicy.org/scans/NYDPH-report.pdf?utm_source=chatgpt.com" target="_blank">and State Evaluations Independent statewide evaluation (2009) found reductions in hospitalization, homelessness, arrests and incarceration for AOT recipients. City evaluation also found the program effective. | |
| Medical Respite | State-funded and H+H-run short-term medical respite beds for people exiting hospitals who are homeless | 75 beds | No NYC Evaluation A systematic review found that similar programs reduce hospital readmissions, inpatient days and admissions, and improve housing outcomes. | |
| TIL (Transitional Independent Living) | Department of Youth and Community Development residential programs for youth (short-term crisis and long-term) | Unknown | No NYC Evaluation | |
| ECUs (Extended Care Units) | H+H hospital-based psychiatric extended-care units. | 60 beds (2024) | NoNYC Evaluation A systematic review of rehab / extended-stay settings found that the most consistent outcome was reduced subsequent inpatient service use after discharge. | |
| Fountain House Clubhouses | Free, voluntary, member-led clubhouse serving ~2,000 adults with serious mental illness | ~2,000 members (2023) | NYC Evaluation An NYU study showed 21% Medicaid cost savings from reduced hospitalizations. | |
| Bridge to Home | H+H program providing noncongregate medical respite / step-down beds | 46 beds (2024) | No NYC Evaluation A systematic review found that these programs reduce hospital readmissions, inpatient days and admissions, and improve housing outcomes. | |
| Housing | ||||
| Safe Havens | Low-barrier, service-rich beds for street-homeless people; placements coordinated via DHS Joint Command Center | ~4,000 beds (2025) City combines this count with stabilization beds. | No NYC Evaluation A Ward Family Foundation evaluation found in another jurisdiction that from 2011-2013, 55% of veteran participants were moved into stable housing | |
| Supportive Housing | Permanent housing with on-site services; mixed funding (City/State/federal); includes scattered-site and congregate | 40,472 units, 94% occupancy (2025) | NYCEvaluation Evaluation found net public cost savings and reduced service use vs. eligible non-tenants; Urban Institute study showed similar findings. | |
| Stabilization Beds | Short-term, low-barrier stabilization sites for unsheltered individuals | City combines this count with Safe Havens. | No NYC Evaluation A systematic review of homelessness interventions, including stabilization beds, was found to outperform other services to improve residential stability. | |
| Drop-in Centers | DHS-contracted centers offering basic services and case management | 9 centers (2025) | No NYC Evaluation | |
| RHY (Runaway and Homeless Youth) | Department of Youth and Community Development shelters for youth / young adults experiencing homelessness | 60 beds (2025) | No NYC Evaluation A Los Angeles, California, study of a similar youth drop center found a positive impact for participants. | |
| Justice Involved | ||||
| JISH (Justice-involved / jail in-reach supportive housing) | Justice-involved / jail in-reach supportive housing (program naming varies) | 120 units (2025) | NYCEvaluation Evaluation found that justice-involved supportive housing significantly reduced cycling between public systems, days spent in jail and shelter, and use of crisis care health services. | |
| Transitional Housing | MOCJ-funded short-term housing options for justice-involved individuals (various sponsors) | 1000 beds (2023) | NYC Evaluation Descriptive data provided by MOCJ show that participants had a lower rearrest rate. | |
| Just Home | Supportive housing initiative for medically vulnerable people leaving custody; funded by H+H and working with HPD and service providers | 83 units | No NYC Evaluation An evaluation of a similar program in Ohio found that participants had greater housing stability and were significantly less likely to be rearrested, convicted or reincarcerated. | |
| Drug Treatment Courts | Statewide problem-solving courts focusing on substance use | Unknown | NYC Evaluation Center for Court Innovation evaluation found that participants were less likely to be arrested. | |
| HOPE (Heroin Overdose Prevention and Education) | Prearraignment diversion program run by the Richmond County District Attorney's Office (Staten Island) | Unknown | NYC Evaluation An MOCJ evaluation found that a Richmond County HOPE pilot reduced recidivism. | |
National models and programs
Programs from across the U.S. that have been referenced as potential models to introduce in New York City.
Case studies from other large cities
| Category | Program Name | Description | City / Jurisdiction | Evaluation |
|---|---|---|---|---|
| Crisis Response and First Response Programs | ||||
| STAR (Support Team Assisted Response) | Embedded in 911 and coordinated by Denver Public Health and Denver 911; staffed by mental-health clinicians and paramedics (not police or fire) | Denver, CO | Denver Evaluation Descriptive data find no police calls, no arrests and no injuries. A CEBP evaluation found no significant impact on nearby serious or violent crimes. | |
| HEART (Holistic Empathetic Assistance Response Teams) | Civilian clinicians and peer responders dispatched through 911 or 311 for nonviolent crises. Data are tracked under the City's racial-equity framework. | Durham, NC | Pilot Evaluation Descriptive data of pilot year show promise and is planned for evaluation. | |
| Albuquerque Community Safety | A stand-alone 911-response department staffed by behavioral-health clinicians, peer support workers and outreach specialists who respond to calls for mental-health, homelessness and substance-use concerns; no police dispatch | Albuquerque, NM | No Formal Evaluation | |
| SCRT (Street Crisis Response Team) | Part of the City's "crisis response continuum." Each team includes a paramedic, behavioral-health clinician and peer specialist responding to behavioral-health 911 calls. | San Francisco, CA | San Francisco Evaluation Evaluation is in process. | |
| CIRCLE (Crisis and Incident Response through Community-Led Engagement) | Civilian outreach teams staffed by community-based organizations that respond to nonemergency 911 calls involving unhoused people and behavioral crises; integrated through 311 and coordinated by the Mayor's Office of Public Safety | Los Angeles, CA | No Formal Evaluation Program data show 14,000 incidents diverted and 1,000 individuals were referred to mental and behavioral services. | |
| Street Response Team | Civilian alternative response program for responding to mental health emergencies | Portland, OR | Portland Evaluation Descriptive evaluation findings found a 3.5% reduction in total calls responded to by police and a 19% reduction in police response. | |
| Behavioral Health Treatment and Hospitalization | ||||
| CMHP (Criminal Mental Health Project) / Miami Model | A comprehensive mental health diversion program built to eliminate the criminalization of mental illness; utilizes prebooking and postbooking jail diversion; employs the SOAR model to expedite access to federal benefits | Miami-Dade County, FL | No Formal Evaluation Descriptive program data find CMHP to provide an effective and cost-efficient solution for individuals with serious mental illness and co-occurring serious mental illness. | |
| Judge Ed Emmett Mental Health Diversion Center | Law enforcement transports individuals identified with mental health needs directly to the Diversion Center instead of jail, based on voluntary participation. The process takes an officer 11 minutes compared to 4 hours for jail booking. 24/7 diversion drop-off for police transporting people in behavioral crisis instead of jail or ER. | Houston / Harris County, TX | Houston Evaluation Evaluation found that program participants who were homeless experienced reductions in psychiatric hospitalizations in the long term, but not short term. | |
| CBH (Community Behavioral Health) | A City-controlled managed-care organization integrating Medicaid behavioral-health dollars into a unified delivery system focused on recovery, housing and harm reduction | Philadelphia, PA | Philadelphia Evaluation External quality review of descriptive data finds improvements in reducing psychiatric hospitalizations. | |
| Crisis Now Framework | 24/7 crisis system with regional crisis call centers, mobile teams and short-term stabilization facilities | Arizona, statewide (Maricopa County pioneer) | No Formal Evaluation An exploratory process evaluation is in progress. | |
| Crisis Response Center (Sequential Intercept Model) | Diversion by law enforcement that uses a "no wrong door" policy, meaning no exclusions based on payer status, intoxication or involuntary status; features a dedicated entrance to expedite law enforcement drop-off, taking officers about 10 minutes | Tucson, AZ | No Formal Evaluation | |
| CM (Contingency Management) | An evidence-based treatment primarily for stimulant use disorders (like cocaine or methamphetamine); uses incentives, often cash payments, for specific positive behaviors such as providing clean drug tests | General practice (e.g., San Francisco pilot) | Systematic Review Review finds CM to be an effective treatment for individuals with opioid use disorder. | |
| MAT (Medication-Assisted Treatment) | Utilizes medications like methadone or buprenorphine (Suboxone) to treat opioid use disorder; can include flexible take-home policies and delivery services to increase access and stability | General practice (e.g., San Francisco) | San Francisco Evaluation Evaluation finds that MAT reduces hospitalizations and improves stability. | |
| MAP (Managed Alcohol Use Program) | Stabilization and harm-reduction intervention for people with alcohol use disorder, sometimes involving managed alcohol programs where clients are given small amounts of alcohol; also known as "wet housing" | General practice (e.g., San Francisco) | Systematic Review Review finds MAPs a promising harm reduction intervention. | |
| Housing | ||||
| HRH (Harm Reduction Housing) | Provides stable living environments without sobriety mandates; offers 24/7 harm reduction supplies, counseling and medical oversight on-site to reduce the risks associated with drug use, such as using alone | Boston, MA | No Formal Evaluation | |
| Temporary Shelter Provision (Winter Shelter Beds) | Provision of additional temporary shelter capacity during the winter months | Los Angeles County, CA | Los Angeles Evaluation A study finds these programs reduce unsheltered homelessness as well as crime and ER visits. | |
| Tiny Cabins / Tiny Homes | Noncongregate, cost-effective interim housing options; San Francisco's first cabin community was established quickly on borrowed private land for temporary use | San Francisco, CA | No Formal Evaluation | |
| Justice Involved | ||||
| LEAD (Let Everyone Advance with Dignity) | Case management diversion for low-level offenses, replacing arrest with community-based care | Seattle, WA (replicated nationally) | North Carolina Evaluation Participants are less likely to have arrests and outpatient behavioral visits as well as higher utilization of medication. | |
Glossary of terms
Systems, agencies and programs
311/911 Systems
311/911 are the City’s call systems consisting of nonemergency (311) and emergency (911) dispatch lines, routing homeless concerns through 311 and psychiatric crises through 911.
988 is the City’s suicide and crisis call system, which can also dispatch DOHMH operated MCT teams to individuals in crisis.
AOT — Assisted Outpatient Treatment (Kendra’s Law)
AOT is authorized by a 1999 State law (Kendra’s Law), consists of court-ordered treatment plans and mandates medication, therapy and case management for individuals with severe illness and treatment noncompliance history. The petition can be filed by a range of individuals including a hospital director, psychiatrist, psychologist, probation officer or family members.
CIDI — Center for Innovation through Data Intelligence
CIDI is the Mayor’s Office data hub. It consists of integrated databases linking City systems and coordinates cross-agency data integration.
DHS — NYC Department of Homeless Services
DHS is the City agency that funds and operates shelter systems, street outreach providers and street outreach nurses, and manages temporary living (e.g., Safe Havens).
DOHMH — NYC Department of Health and Mental Hygiene
DOHMH is the City agency that operates behavioral health programs, deploys mobile crisis teams and coordinates mental health strategy with H+H and nonprofits.
H+H — NYC Health + Hospitals
H+H is the City’s public hospital system, which operates emergency departments, CPEPs, Correctional Health Services at Rikers and different treatment and transition programs (e.g., Just Home).
HUD — U.S. Department of Housing and Urban Development
HUD is the federal agency that funds housing vouchers and homelessness assistance programs including Continuum of Care and HUD-VASH.
MOCJ — Mayor’s Office of Criminal Justice
MOCJ is the mayor’s coordinating office for criminal justice policy. It manages diversion and reentry initiatives and oversees supportive housing programs for justice-involved individuals.
OASAS — Office of Addiction Services and Supports
OASAS is the New York State agency that funds and operates substance use treatment programs, funds harm reduction and recovery services and oversees addiction treatment policy statewide.
OMH — New York State Office of Mental Health
OMH is the New York State agency that funds and operates psychiatric programs and institutions and oversees mental health policy statewide.
OTDA — Office of Temporary and Disability Assistance
OTDA is the State agency that administers emergency aid programs, funds supportive housing grants and oversees temporary assistance policy.
SAMHSA — Substance Abuse and Mental Health Services Administration
SAMHSA is the federal agency that funds behavioral health block grants, supports State and local programs and sets national behavioral health policy.
VA — U.S. Department of Veterans Affairs
VA is the federal agency that operates veteran health facilities, runs HUD-VASH housing programs, and provides mental health services for veterans.
Crisis outreach and treatment programs
ACT — Assertive Community Treatment
ACT teams are operated by the New York State Office of Mental Health. They consist of psychiatrists, nurses, social workers and peer specialists, and provide 24/7 field-based treatment for adults with severe mental illness.
B-HEARD — Behavioral Health Emergency Assistance Response Division
B-HEARD is a City pilot program staffed by FDNY and H+H. It consists of unarmed clinician-EMT teams and responds to mental health 911 calls in select precincts.
CPEP — Comprehensive Psychiatric Emergency Program
CPEP are 24/7 psychiatric emergency programs funded by the State and operated by City hospitals, providing critical crisis and evaluation services to individuals with serious mental illness.
CTI - Critical Time Intervention
CTI, founded in New York City, is a time-limited, evidence-based case management model employed by SOS teams that provides intensive support during periods of transition for individuals in crisis and cycling between systems.
EOL — End of Line
EOL are multiagency teams working at end-of-line stations as part of the Subway Safety Plan, connecting individuals to services.
FACT — Forensic Assertive Community Treatment
FACT teams are a specialized ACT model. They consist of behavioral health clinicians and criminal justice liaisons and provide integrated treatment and supervision for people with serious mental illness involved in the justice system.
Free, voluntary, member-led spaces administered and run by Fountain House, serving adults with serious mental illness in New York City.
IMT — Intensive Mobile Treatment
IMT teams are operated by DOHMH. They consist of clinical staff similar to ACT composition and treat people with serious mental illness who are homeless, recently incarcerated or repeatedly hospitalized.
MCTs — Mobile Crisis Teams
MCTs are operated by DOHMH. They consist of clinician-led rapid-response units and respond to psychiatric crises dispatched through 988 or hospital networks.
Medical respite is funded by the State and operated by H+H, offering short-term medical respite beds for people exiting hospitals who are homeless.
PATH — Police and Transit Homelessness Co-response Program
PATH operates primarily overnight; consists of joint teams from NYPD, DHS and H+H; and responds to homelessness in subway and transit systems.
SCOUT — Subway Clinician Outreach Unit Teams
SCOUT operates primarily during daytime hours, consists of clinician-led teams partnered with MTA and DHS, and provides outreach in the subway system.
Situation Tables
Cross-agency meetings (police, clinicians, outreach, housing) reviewing the highest-risk individuals and coordinating targeted interventions.
SOS Teams — Safe Options Support
SOS teams are funded by OMH, consist of multidisciplinary outreach workers and conduct street outreach to connect unsheltered individuals to housing and other services.
Housing and shelter programs
JISH — Justice-Involved Supportive Housing
JISH is a housing model that consists of apartments with intensive supervision and clinical services both for justice-involved individuals with serious mental illness exiting jail or prison.
Safe Havens, funded and operated by DHS, are low-threshold residential housing for street homeless individuals. They consist of single rooms with reduced rules (pets allowed, no curfews, couples permitted) and serve a high-need population who decline traditional shelters.
Stabilization beds, funded and operated by DHS, are short-term, low-threshold beds for individuals transitioning from the street to more permanent housing. They are typically less service-intensive than Safe Havens.
Supportive housing is permanent affordable housing consisting of independent units with on-site case management and clinical services, and serving people with mental illness, disabilities or chronic homelessness.
Street-to-Housing is a pilot run by the Volunteers of America, consisting of single-room units with on-site supports to place individuals directly from the street into housing without shelter system entry.
Legal frameworks and mental hygiene laws
MHL 9.41 (Police Removal)
MHL 9.41 is a State mental hygiene law provision authorizing NYPD officers to transport individuals for psychiatric evaluation. It applies when someone poses danger to themselves or others or cannot meet basic needs.
MHL 9.58 (Clinical Removal)
MHL 9.58 is a State mental hygiene law provision authorizing licensed mental health professionals to order transport to hospitals. It applies under similar danger criteria as 9.41.
These are State psychiatric hospitalization statutes consisting of progressive commitment periods. They require escalating levels of clinical and judicial authorization:
- 9.40: Up to 72-hour evaluation
- 9.39: Up to 15-day emergency hospitalization
- 9.27 / 9.37: 60-day commitment with physician certification
- 9.33: Court-ordered extended hospitalization
Kendra’s Law is a 1999 State statute. It established AOT following a homicide by a person with untreated schizophrenia and authorizes court-ordered outpatient treatment.
AB 210 (California)
AB 210 is California legislation. It authorizes data sharing across health, housing and safety providers with confidentiality protections; it is cited as a model for cross-system coordination.
Data and coordination initiatives
CAPS — Coordinated Assessment and Placement System
CAPS, operated by New York City’s Continuum of Care (CoC), is the City’s internal database for matching individuals to supportive housing and other placements.
CoC — Continuum of Care
New York City’s CoC is the HUD-mandated coordination system that consists of City agencies and nonprofit providers. It allocates federal homelessness funding and organizes service delivery.
StreetSmart is DHS’ digital platform. It consists of a database tracking outreach contacts by name and records engagement and progress of unsheltered individuals.
SPOA — Single Point of Access
SPOA, operated by DOHMH, helps connect people with serious mental illness to the appropriate providers.
Top 50 lists are internal by-name rosters that identify the most vulnerable or frequently encountered individuals. They are used to prioritize interventions in subways and on streets.
Funding and contracting
Outcome-based contracting is a proposed payment model for New York City nonprofits. It ties funding to results like housing stability or reduced crisis recurrence and shifts from activity-based to results-based reimbursement.
Bundled payments are a proposed funding structure. They consist of single-payment streams covering all services for an individual (housing, care, outreach) and make one provider accountable for coordination.
Prompt Pay Standard
The prompt pay standard is a proposed contracting reform that requires timely payments to nonprofit providers and aims to prevent cash-flow crises that delay service delivery.
Clinical and behavioral concepts
SMI — Serious Mental Illness
SMI is a diagnosable mental, behavioral or emotional disorder — such as bipolar disorder, major depressive disorder and schizophrenia — that substantially interferes with a person’s life and ability to function.
Co-Occurring Disorders / Dual Diagnosis
“Co-occurring disorders” refers to concurrent mental illness and substance use disorder. Common among street homeless populations, co-occurring disorders require integrated treatment approaches.
Anosognosia is a psychiatric symptom consisting of lack of awareness of one’s own mental illness. It contributes to treatment refusal in disorders like schizophrenia.
Psychosis / Drug-Induced Psychosis
Psychosis is a mental state involving loss of contact with reality. It can be triggered or worsened by substance use and includes symptoms like hallucinations and delusions.
TBI — Traumatic Brain Injury
TBI is a neurological injury caused by external physical trauma to the head due to assault, falls and accidents, ranging from mild concussions to severe brain damage.
════════════════════════════════════════
New York is entering an historic and pivotal transition. Mayor-elect Mamdani faces big problems on housing, safety, mental health, transit, and more.
Vital City is uniquely positioned to offer clear, practical guidance rooted in evidence. Ideas that could actually be implemented and work.
But to meet this moment, we need to grow.
That’s why, this year, for the first time, we’re asking our readers to support Vital City directly. We’re aiming for 700 inaugural supporters by December 31.
Your support will help us expand our editorial capacity, strengthen our operational support, and continue delivering thoughtful, relevant and informative work in 2026.
If this article informed your thinking, challenged you, or helped you understand the city more clearly, please consider supporting the work behind it.
Make your tax-deductible gift and help us reach 700 supporters.
Vital CityThis is one of three supporting documents connected to Vital City’s recommendations on serious mental illness and homelessness, “What To Do (and Not To Do) About People in Crisis on Streets and Subways.” Find "What the Data Show" here and "Case Studies from Other Large Cities" here.
Download PDF Print PDF
A profile of the population
On any given night, about 4,000 people are living on the street in New York City. That figure, drawn from a point-in-time count, understates the scale of the problem: Because people cycle in and out of unsheltered homelessness, the number of unique individuals affected over the course of a year is likely much higher.
New York isn’t alone among American cities in facing this issue: In fact, the scale of the problem is not especially bad by some measures. Unlike most large U.S. cities, which have larger unsheltered populations as a portion of all homeless individuals, New York guarantees a temporary bed to anyone who needs one. This legal right to shelter and the network of facilities that go with it keep roughly 95% of homeless people indoors, leaving a concentrated group with acute needs and a demonstrated reluctance to accept a shelter bed (or sometimes even a nonshelter bed) on the street. In a dense city, the visibility of this troubled population can fuel perceptions of disorder and personal risk that exceed the problem’s actual scale.
Within this population, needs and circumstances vary widely. Many people grapple with serious mental illness and/or substance use disorders. Some have conditions such as schizophrenia or bipolar disorder that respond to sustained treatment and support; others live with personality disorders that require long-term psychosocial care. Co-occurring substance use is common and complicates engagement; to the untrained eye, a seeming mental illness crisis may in fact be drug-induced psychosis that wears off when the drug’s effects subside. Another complicating factor is traumatic brain injuries (TBI), which is estimated to affect more than half of people experiencing homelessness.
While it’s true that a person who is homeless is more likely to be a victim than a perpetrator, unstable people living on the street can indeed pose serious safety risks. In 2024, 1,285 street-homeless people were arrested for assault, a rate more than 20 times that of the total city population. Yet criminal offending isn’t a factor in prioritizing who gets the most focused attention, even on the City’s “Top 50” lists — the informal name for the internal rosters used to coordinate work on the most serious subway and street cases.
Particular crimes committed by these individuals loom large and heighten public fear. There was the fatal 2022 subway shoving of Michelle Go in the Times Square-42nd Street station and, more recently, the 2024 stabbing spree across Manhattan that left three people dead. Untreated illness and addiction also often manifest as erratic behavior that many experience as threatening. For the individuals themselves, surviving in public without effective care means worsening health, criminal justice involvement, vulnerability to victimization and repeated emergencies, often resulting in an unbroken cycle through the street, shelter, ER and jail akin to those Dr. Ross MacDonald identified in his analysis of Rikers Island “hot spotters.”
What government currently does about the challenge
Billions of public dollars are spent each year on both homelessness and behavioral health, yet this specific cohort remains too disconnected from sustained attention, typically cycling through brief and redundant contacts with police, hospitals and shelters before returning to the street. The visible churn convinces the public that government cannot care for the most vulnerable people or maintain order in common spaces.
Of course, even if everything ran like clockwork, there would be crises and failures. These are bedevilingly difficult cases to manage. Government and nonprofit providers put an enormous amount of thought and commitment into addressing difficult circumstances. But far too much effort, money and time are squandered because multiple systems operate in parallel — the police, 911 and 311, EMS, homeless-services outreach teams, public hospitals and nonprofit providers. Each has different mandates, funding sources, data systems and protocols. Handoffs are inconsistent; information is siloed; continuous case management and accountability are absent. Outreach teams often lose track of clients once cases move outside their geography or specialty. Hospitals frequently discharge psychiatric patients back to the street after brief observation because longer-stay treatment beds and step-down options are scarce. Judges who see mentally ill or drug-addicted defendants have few viable pathways to secure treatment instead of jail because effective programs have limited slots. At Rikers Island, an estimated one-third of people admitted in 2023 were homeless before arrest; upon release, only about 3% of detainees with serious mental illness were connected to supportive housing, with most returning to shelters or the street.
1. Contact with individuals in crisis and what follows
It’s not easy to get one’s arms around all the opportunities for official intervention — the many ways in which a seriously mentally ill or otherwise unstable homeless person living on the street encounters police, mental health professionals, social workers and others — but it’s important to try to see the current tangled system in all its complexity.
There are two primary ways unsheltered individuals in public spaces with serious mental illness will make contact with the system: police dispatch (i.e., 911) in response to a crisis, and outreach teams (sometimes civilian, sometimes a mix of police and civilian) that initiate contact with individuals even when there is no reported emergency.
After an encounter, police (usually) can transport an individual involuntarily to a hospital for a psychiatric assessment if they’re in psychiatric distress and qualify for transport, which under the law is defined as presenting a danger to themselves or others, a definition that includes the inability to take care of their own basic needs. If the person does not qualify for involuntary transport, then they could either be arrested if alleged to engage in criminal activity, or offered to be connected to different services (e.g., housing).
Not all people who live on the street are in the throes of crisis, but crises happen with some level of frequency. New York City’s behavioral health crisis response still defaults to 911, with police and EMS as the primary responders. The NYPD fields more than 150,000 calls each year involving psychiatric distress (a number that includes people who are housed). Police are usually present for three reasons: the possibility of violence, social workers’ preference for backup in unpredictable situations and the legal requirement that only police can carry out involuntary transports.
Alongside 911, 311 serves as the City’s nonemergency intake and routing line for homeless-related concerns. In 2024, the DHS (Department of Homeless Services) handled about two-thirds of these calls, and the NYPD handled the remaining third. Among the City’s outreach efforts, co-response teams — the MTA’s clinician-led SCOUT (Subway Co-Response Outreach Teams), a daytime program conducted in partnership with DHS, and PATH (Partnership Assistance for Transit Homelessness), an overnight program led by the NYPD, DHS and the City’s public hospital system — are among the most recently conceived initiatives. These teams work to actively find and engage people in distress instead of waiting for a call to come in. Their models pair mental health clinicians with police officers to handle crises together, combining treatment expertise with public safety backup. (Though they are expanding, they remain small: SCOUT began with two pilot teams and is slated to reach roughly 10 by year’s end. PATH does not publish similar numbers.)
There is growing interest, including by Mayor-elect Mamdani, in the City’s B-HEARD (Behavioral Health Emergency Assistance Response Division) pilot — unarmed teams of clinicians and EMTs dispatched to eligible mental health 911 calls instead of police — as an alternative. The program’s current footprint in 31 precincts (of 78) and roughly 15,000 calls handled in 2024 remains a small amount relative to need. And, as with many if not all of the programs and approaches, there has been no reliable (or publicly available) assessment of what kinds of problems B-HEARD is effective at addressing and what it is not.
B-HEARD was modeled on CAHOOTS in Eugene, Oregon, pairing health professionals with responders for behavioral health crises, but it does not fulfill the same role. CAHOOTS (Crisis Assistance Helping Out On The Streets) combines crisis response with sustained, proactive outreach in the community, while in New York City that outreach is handled by separate street outreach teams rather than B-HEARD. B-HEARD focuses on reacting to selected 911 calls during limited hours instead of serving as a default, community-based alternative. The result is often trading one type of responder for another rather than changing how and when help reaches people.
Both strategies, B-HEARD and involuntary transports, suffer from an absence of sufficient publicly reported outcome measures to tell policymakers whether these responses actually improve stability, reduce repeat crises and connect people to care. This makes it difficult to evaluate their effects and determine whether they’re as effective as other nonpolice alternative response programs (e.g., Denver’s STAR (Support Team Assisted Response)).
This raises a crucial recurring theme: The orientation of the current system — to deal mainly with point-in-time crises instead of sustained attention to a particular person throughout their life course — means that neither government nor anyone else with responsibility has a panoramic view of how any one individual is doing after the crisis.
Much of the public reporting on these efforts remains focused on activity — contacts, referrals and transports. But there is little known about durable results such as housing retention, reduced crisis recurrence or diversion from the justice system. Without those measures, it is difficult to know whether scaling up is translating into lasting impact.
By contrast, several civilian outreach models have expanded in recent years. State OMH’s (Office of Mental Health’s) SOS (Safe Options Support) teams grew from four to 20 between 2022 and 2025, with press coverage citing State data showing 800 people placed into permanent housing in New York City from April 2022 to April 2025 after 58,000 engagements. SOS teams are multidisciplinary groups (clinicians, peers and care managers) who do persistent, field-based outreach both topside and underground, stay with people to help navigate paperwork and appointments, and broker placements into Safe Haven / stabilization beds and supportive or permanent housing.
The City has made numerous concerted efforts to knit together the fragmented system and focus on those in greatest need. One example is the StreetSmart application. StreetSmart, a project of the Department of Homeless Services, is a digital by-name list — a shared, person-specific roster used by City-contracted outreach providers to track individuals living unsheltered and to record engagements and progress over time. This is a real innovation. Unfortunately, it excludes many nonprofits that are not under City contract and therefore are not bound by the City’s privacy rules. Health, housing and police data are not integrated, and health-privacy rules restrict certain types of data sharing. These gaps make it difficult to measure outcomes or coordinate care effectively.
2. Involuntary Transport & Hospitalization
After a response or outreach team makes contact with an unsheltered individual, the next step is assessing whether the individual is in psychiatric distress. If an individual is in crisis, both police and clinicians have the power of involuntary removal to a hospital (under New York State Mental Hygiene Law Sections 9.41 and 9.58). The current administration has leaned into involuntary transport to hospitals under the Mental Hygiene Law as part of its strategy. It’s unclear whether expanded use of involuntary transport will break existing cycles or worsen them — an uncertainty the City should resolve through rigorous evaluation. It is critical that the City learn what the results are so that it can determine how most effectively to implement the law. In 2024, police initiated about 7,000 involuntary transports (Section 9.41), roughly two-thirds of which originated from 911 calls. Clinicians accounted for another 661 (Section 9.58). There is no public accounting of whether the removals in 2024 are more or fewer than in the past. Also, while 57% of individuals transported pursuant to an order issued by a clinician (9.58) are admitted, there is no public reporting on how many individuals are admitted into psychiatric care after a police transport (9.41).
Once at the hospital, a person can be held for a short evaluation under Section 9.40, typically lasting up to 72 hours. This evaluation typically occurs in a CPEP (Comprehensive Psychiatric Emergency Program) unit, the designated psychiatric emergency department. If doctors determine that the person still needs inpatient care, they may be admitted under Section 9.39, which allows up to 15 days of emergency hospitalization. For people who continue to need treatment, the hospital can extend the stay under Sections 9.27 or 9.37, based on certification by doctors and a psychiatrist, for up to 60 days. If more time is required, the hospital must seek a court order under Section 9.33 to keep the person longer. A small number of extended-care units provide about 90 to 120 days of treatment, and there are also medical respite beds for patients with physical health needs.
If an individual is not admitted or discharged, options are extremely limited. Even if admitted to psychiatric care, individuals may face prolonged waits in emergency departments due to psychiatric boarding — when patients remain in the ER for extended periods because no inpatient psychiatric beds are available. There are few alternatives for those not admitted and difficulty accessing long-term or supportive housing options to ensure stability after discharge.
It is also worth noting that some constraints concerning long-term psychiatric care stem from State and federal financing and regulatory rules that limit what care is available and for how long, notably Medicaid’s IMD exclusion, which generally prevents federal funding for adults aged 21 to 64 receiving care in psychiatric facilities with more than 16 beds.
3. Treatment and other services
While improving the initial response to individuals in crisis is often presented as central to solving the problem, changing who initially responds when a crisis happens is not enough. If an individual is not admitted to a hospital or arrested, what happens next is typically what matters most. Same-day clinical access? Intensive Mobile Treatment (IMT), which provides support and treatment in streets, shelters and public spaces? Detox and step-down care? Supportive housing with services? And is there a smooth transition to this help?
Without the right resources at the right moment, most encounters eventually result in the person cycling back to emergency rooms, shelters or the street. B-HEARD can reduce police call volume, and it might reduce the risk of a given incident escalating, but it does not address the underlying problem of “What next?” or necessarily address the underlying problem motivating the report.
Again, the “What next?” question rears its head. The City does not publish systemwide data on how many of the police-initiated transports result in admission or for how long or what happened to the person upon release.
Treatment following inpatient hospitalization is crucial. Assisted Outpatient Treatment, which is court-ordered under Kendra’s Law, gives individuals psychiatric treatment plans to follow once they’ve been stabilized. It is an important piece of the puzzle, especially given evaluations both within and outside of New York that have found it to be effective in reducing psychiatric episodes and improved outcomes.
OMH’s Assertive Community Treatment (ACT) shows promising evidence of stabilizing housing and reducing psychiatric crises. ACT serves adults with the highest, ongoing psychiatric needs; multidisciplinary teams provide community-based care with small caseloads, 24/7 crisis coverage and time-unlimited support for as long as the person benefits. Similar to ACT, the Mayor’s Office of Community Mental Health has implemented IMT teams that serve adults with serious mental illness who are often street- or shelter-based, recently incarcerated or repeatedly hospitalized. IMTs meet people in the field at points of crisis or transition (street, ER or jail/prison discharge) and remain engaged as long as clinically needed, often many months, until a step-down is appropriate. For IMT, however, a 2024 City comptroller audit found issues with tracking outcomes and program management. Incarceration data were not regularly tracked and treatment engagement was inconsistently measured. Reviews of providers varied in quality, follow-up on corrective actions lagged and the program still lacks transparent, system-level reporting to demonstrate durable outcomes — a gap also highlighted by a New York Times investigation into the City’s fragmented mental health response. However, mobile treatment capacity is constrained: The City funds 31 IMT teams serving fewer than 1,000 clients, with similar pressure on State-funded ACT teams.
It is also worth noting that some constraints concerning long-term psychiatric care stem from State and federal financing and regulatory rules that limit what care is available and for how long, notably Medicaid’s IMD exclusion, which generally prevents federal funding for adults aged 21 to 64 receiving care in psychiatric facilities with more than 16 beds.
4. Shelter and housing placements
Housing must be a central part of the approach to stabilizing people who lack it and are on the verge of psychiatric crisis. But even when the City can identify and reach people with the highest needs, individuals are typically routed to places that are, by design, temporary, including ERs; crisis respite centers; Safe Havens, which are low-barrier, small-scale programs that provide private rooms and flexible rules for people coming directly from the street, who often resist traditional shelters due to their safety records, strict curfews, sobriety requirements and other rules; stabilization beds, which are low-threshold beds for a high-functioning population; general shelters; or short jail stays.
Some of these placement failures could be addressed by increasing Safe Haven and stabilization beds, speeding documentation, expanding mobile treatment capacity and improving handoffs.
Supportive housing — permanent affordable apartments with on-site services — is by far the most crucial component of any system to help this population. Yet today, approvals do not reliably translate into placements for unsheltered individuals. Despite the strong evidence base concerning the effectiveness of supportive-housing programs, outreach programs have struggled to secure housing placements. In 2024, outreach teams secured supportive-housing approvals for 955 unsheltered people, but only 175 (18%) obtained a unit, often due to process barriers; at the same time, more than 4,100 supportive-housing units sat vacant. Unsheltered homeless people don’t just suffer from mental illness and addiction; they lack, and need, some community. Here, clubhouses like those run by Fountain House have helpfully expanded in recent years, giving individuals a psychologically healthy place to go during the day and a connection with related services. A person who is connected with others is more likely to get the help they need when they need it.
5. Criminal justice interactions and what follow
In some instances, the initial interaction with police stems from criminal behavior. In 2024, NYPD recorded 15,274 arrests of unsheltered New Yorkers. Most commonly, these arrests are for petit larceny, misdemeanor drug offenses or assault charges.
When a police officer makes an arrest, the defendant is charged and brought before a judge for arraignment. At arraignment, the judge has the option to release the individual on their own recognizance pending the resolution of the case, release with certain conditions or set bail and hold the individual in detention. In the case of homeless individuals, lack of stable housing is sometimes considered by judges in determining risk of flight, and any amount of bail could effectively result in being held in jail pending trial if they are unable to afford it.
For individuals who appear to have a serious mental illness, judges will sometimes order an exam under Criminal Procedure Law 730 (”730 exam”), to determine whether the individual is an incapacitated person — a defendant who “as a result of mental disease or defect lacks capacity to understand the proceedings against him or to assist in his own defense.” For underlying misdemeanor charges, a finding of incapacitation results in the dismissal of the underlying misdemeanor case as well as care and treatment in an appropriate institution for up to 90 days. For felony cases, longer orders of commitment are possible, and the status of the underlying criminal case will depend on whether or not it is ultimately indicted by the prosecutor. In cases of an indicted felony, the individual can be held in a State forensic psychiatric facility for up to two-thirds of the maximum sentence if the patient had been found guilty of the underlying felony. It is also worth noting that the process of 730 exams can often lead to many case delays and a much lengthier stay of incarceration or time in a psychiatric facility for individuals with serious mental illness.
In the absence of a 730 exam, prosecutors still have many tools at their disposal for individuals living with serious mental illness and/or substance use disorder. Included in these options are mental health and drug-treatment courts, as well as the possibility for treatment as a condition of a plea deal or as part of a final sentence.
For those who are living with serious mental illness who are held in jail, there are specialized units called CAPS (Clinical Alternative to Punitive Segregation) units, as well as therapeutic beds, which provide treatment for individuals with serious mental illness while incarcerated. If convicted of a crime and transferred to State custody, there is a continuum of care for incarcerated individuals offered by OMH, including the Central New York Psychiatric Center as well a statewide network of clinics, crisis beds and intermediate care program beds.
Upon release, reentry services are available through nonprofits, NYC Health + Hospitals programs and other City programs, such as the Community Justice Reentry Network, that provide a variety of connections to treatment, care, housing and employment resources.
These are hard cases. Providing services to people living with mental illness is much more complex than providing food to the hungry. Many people of greatest concern do not realize they are ill, a condition known as anosognosia. Others carry trauma or deep distrust of systems and may refuse help repeatedly. Even a well-functioning system is likely to fail more often than it succeeds. But today, batting averages are dangerously low. The system’s flaws are clear: Information is siloed, coordination across agencies is thin, services are poorly matched to need and unevenly distributed, connections are not sustained as symptoms change over time and there is little culture of disciplined self-assessment or course correction. As with every other aspect of engagement with those living with serious mental illness and/or homelessness, the description of the system process does not always align perfectly with delivery. Often there are not enough services, treatment programs, beds or housing options to meet the needs of the individuals these were created to help.
Appendices
NYC homelessness & mental health budget (2024)
| Agency | Line Items | Amounts (2024) |
|---|---|---|
| DHS | Outreach, Drop-In, Reception | $303.7M |
| DHS | Family Shelter Operations, Intake, Administration | $1.1B |
| DHS | Adult Shelter Operations, Intake, Administration | $969.16M |
| DOHMH | Mental Health Services | $601.56M |
| DOHMH | Alcohol and Drug Prevention, Care and Treatment | $153M |
| DOHMH | Developmental Disabilities | $10M |
| DOHMH | Administration | $52M |
| H+H | Correctional Health Services | $285M |
| H+H | B-HEARD | $13M |
| H+H | Mental Health Service Corps | $12M |
| H+H | Just Home | $1M |
| H+H | DOHMH (Transfer) | $37M |
| FDNY | B-HEARD | - |
| FDNY | Emergency Medical Services | $427M |
| OTI/311 | 311 | $61M |
| OTI/311 | 911 | $101M |
| OTI/311 | Administration, Operations | $66M |
| NYPD | Transit | $291M |
| NYPD | Training | $136M |
| TOTAL | $4.62B | |
| TOTAL | $10.4B | |
The evidence backing various policy approaches
The evidence table below does not attempt to rate the level of evidence for the programs indicated. Instead, it aims to be illustrative and provide an overview of what data and research are available for the programs.
NYC programs: evidence and evaluation
| Category | Program Name | Description | Size and Stats | Evaluation |
|---|---|---|---|---|
| Crisis Response and First Response Programs | ||||
| B-HEARD | Behavioral Health Emergency Assistance Response Division: health and mental health-only response to 911 calls; operated by FDNY EMS and H+H | 33,000 responses citywide (2024) | NYC Evaluation City Council evaluation found 88% of calls were resolved without police, EMS or hospital transport, with higher success in non-housing conditions. | |
| Subway Safety (Subway Safety Unit) | Operation to clear the subway of homeless people, involving NYPD and social workers (initially a temporary NYPD pilot); homeless people relocated to shelters and/or hospitalized; program has been the subject of legal challenges | 1800 outreaches 1150 subway removals (2024-to-date) | NYC Evaluation No city evaluation has been performed; advocacy groups have raised concerns about quality of outreach. | |
| Directive 25 (NYPD Directive 25) | Directed "street homeless" individuals with mental illness to be involuntarily hospitalized. | Unknown citywide At least 2000 interactions (2023-to-date) | NYC Evaluation No city evaluation has been performed; advocacy groups have raised concerns about implementation quality and protections against involuntary care. | |
| MCTs (Mobile Crisis Teams) | Nonpolice mental health response for individuals in crisis; may be accessed via 311/988 | 200,000 responses citywide (2023) | NYC Evaluation An evaluation of a different city effort resulted in reductions of arrests, psychiatric hospitalizations and emergency room visits. | |
| CPEPs (Comprehensive Psychiatric Emergency Programs) | State-regulated 24/7 psychiatric emergency programs; recent State capital expansion initiative | 11 programs through H+H (2024), additional programs through private hospitals | No NYC Evaluation An evaluation of a similar program in the Midwest finds effective results. | |
| AOT (Assisted Outpatient Treatment) | Court-ordered outpatient treatment administered via OMH/localities | 47,000 investigations, 96% petitions granted | NYC a href="https://static.prisonpolicy.org/scans/NYDPH-report.pdf?utm_source=chatgpt.com" target="_blank"> and State Evaluations Independent statewide evaluation (2009) found reductions in hospitalization, homelessness, arrests and incarceration for AOT recipients. City evaluation also found the program effective. | |
| Medical Respite | State-funded and H+H-run short-term medical respite beds for people exiting hospitals who are homeless | 75 beds | No NYC Evaluation A systematic review found that similar programs reduce hospital readmissions, inpatient days and admissions, and improve housing outcomes. | |
| TIL (Transitional Independent Living) | Department of Youth and Community Development residential programs for youth (short-term crisis and long-term) | Unknown | No NYC Evaluation | |
| ECUs (Extended Care Units) | H+H hospital-based psychiatric extended-care units. | 60 beds (2024) | No NYC Evaluation A systematic review of rehab / extended-stay settings found that the most consistent outcome was reduced subsequent inpatient service use after discharge. | |
| Fountain House Clubhouses | Free, voluntary, member-led clubhouse serving ~2,000 adults with serious mental illness | ~2,000 members (2023) | NYC Evaluation An NYU study showed 21% Medicaid cost savings from reduced hospitalizations. | |
| Bridge to Home | H+H program providing noncongregate medical respite / step-down beds | 46 beds (2024) | No NYC Evaluation A systematic review found that these programs reduce hospital readmissions, inpatient days and admissions, and improve housing outcomes. | |
| Housing | ||||
| Safe Havens | Low-barrier, service-rich beds for street-homeless people; placements coordinated via DHS Joint Command Center | ~4,000 beds (2025) City combines this count with stabilization beds. | No NYC Evaluation A Ward Family Foundation evaluation found in another jurisdiction that from 2011-2013, 55% of veteran participants were moved into stable housing | |
| Supportive Housing | Permanent housing with on-site services; mixed funding (City/State/federal); includes scattered-site and congregate | 40,472 units, 94% occupancy (2025) | NYC Evaluation Evaluation found net public cost savings and reduced service use vs. eligible non-tenants; Urban Institute study showed similar findings. | |
| Stabilization Beds | Short-term, low-barrier stabilization sites for unsheltered individuals | City combines this count with Safe Havens. | No NYC Evaluation A systematic review of homelessness interventions, including stabilization beds, was found to outperform other services to improve residential stability. | |
| Drop-in Centers | DHS-contracted centers offering basic services and case management | 9 centers (2025) | No NYC Evaluation | |
| RHY (Runaway and Homeless Youth) | Department of Youth and Community Development shelters for youth / young adults experiencing homelessness | 60 beds (2025) | No NYC Evaluation A Los Angeles, California, study of a similar youth drop center found a positive impact for participants. | |
| Justice Involved | ||||
| JISH (Justice-involved / jail in-reach supportive housing) | Justice-involved / jail in-reach supportive housing (program naming varies) | 120 units (2025) | NYC Evaluation Evaluation found that justice-involved supportive housing significantly reduced cycling between public systems, days spent in jail and shelter, and use of crisis care health services. | |
| Transitional Housing | MOCJ-funded short-term housing options for justice-involved individuals (various sponsors) | 1000 beds (2023) | NYC Evaluation Descriptive data provided by MOCJ show that participants had a lower rearrest rate. | |
| Just Home | Supportive housing initiative for medically vulnerable people leaving custody; funded by H+H and working with HPD and service providers | 83 units | No NYC Evaluation An evaluation of a similar program in Ohio found that participants had greater housing stability and were significantly less likely to be rearrested, convicted or reincarcerated. | |
| Drug Treatment Courts | Statewide problem-solving courts focusing on substance use | Unknown | NYC Evaluation Center for Court Innovation evaluation found that participants were less likely to be arrested. | |
| HOPE (Heroin Overdose Prevention and Education) | Prearraignment diversion program run by the Richmond County District Attorney's Office (Staten Island) | Unknown | NYC Evaluation An MOCJ evaluation found that a Richmond County HOPE pilot reduced recidivism. | |
National models and programs
Programs from across the U.S. that have been referenced as potential models to introduce in New York City.
Case studies from other large cities
| Category | Program Name | Description | City / Jurisdiction | Evaluation |
|---|---|---|---|---|
| Crisis Response and First Response Programs | ||||
| STAR (Support Team Assisted Response) | Embedded in 911 and coordinated by Denver Public Health and Denver 911; staffed by mental-health clinicians and paramedics (not police or fire) | Denver, CO | Denver Evaluation Descriptive data find no police calls, no arrests and no injuries. A CEBP evaluation found no significant impact on nearby serious or violent crimes. | |
| HEART (Holistic Empathetic Assistance Response Teams) | Civilian clinicians and peer responders dispatched through 911 or 311 for nonviolent crises. Data are tracked under the City's racial-equity framework. | Durham, NC | Pilot Evaluation Descriptive data of pilot year show promise and is planned for evaluation. | |
| Albuquerque Community Safety | A stand-alone 911-response department staffed by behavioral-health clinicians, peer support workers and outreach specialists who respond to calls for mental-health, homelessness and substance-use concerns; no police dispatch | Albuquerque, NM | No Formal Evaluation | |
| SCRT (Street Crisis Response Team) | Part of the City's "crisis response continuum." Each team includes a paramedic, behavioral-health clinician and peer specialist responding to behavioral-health 911 calls. | San Francisco, CA | San Francisco Evaluation Evaluation is in process. | |
| CIRCLE (Crisis and Incident Response through Community-Led Engagement) | Civilian outreach teams staffed by community-based organizations that respond to nonemergency 911 calls involving unhoused people and behavioral crises; integrated through 311 and coordinated by the Mayor's Office of Public Safety | Los Angeles, CA | No Formal Evaluation Program data show 14,000 incidents diverted and 1,000 individuals were referred to mental and behavioral services. | |
| Street Response Team | Civilian alternative response program for responding to mental health emergencies | Portland, OR | Portland Evaluation Descriptive evaluation findings found a 3.5% reduction in total calls responded to by police and a 19% reduction in police response. | |
| Behavioral Health Treatment and Hospitalization | ||||
| CMHP (Criminal Mental Health Project) / Miami Model | A comprehensive mental health diversion program built to eliminate the criminalization of mental illness; utilizes prebooking and postbooking jail diversion; employs the SOAR model to expedite access to federal benefits | Miami-Dade County, FL | No Formal Evaluation Descriptive program data find CMHP to provide an effective and cost-efficient solution for individuals with serious mental illness and co-occurring serious mental illness. | |
| Judge Ed Emmett Mental Health Diversion Center | Law enforcement transports individuals identified with mental health needs directly to the Diversion Center instead of jail, based on voluntary participation. The process takes an officer 11 minutes compared to 4 hours for jail booking. 24/7 diversion drop-off for police transporting people in behavioral crisis instead of jail or ER. | Houston / Harris County, TX | Houston Evaluation Evaluation found that program participants who were homeless experienced reductions in psychiatric hospitalizations in the long term, but not short term. | |
| CBH (Community Behavioral Health) | A City-controlled managed-care organization integrating Medicaid behavioral-health dollars into a unified delivery system focused on recovery, housing and harm reduction | Philadelphia, PA | Philadelphia Evaluation External quality review of descriptive data finds improvements in reducing psychiatric hospitalizations. | |
| Crisis Now Framework | 24/7 crisis system with regional crisis call centers, mobile teams and short-term stabilization facilities | Arizona, statewide (Maricopa County pioneer) | No Formal Evaluation An exploratory process evaluation is in progress. | |
| Crisis Response Center (Sequential Intercept Model) | Diversion by law enforcement that uses a "no wrong door" policy, meaning no exclusions based on payer status, intoxication or involuntary status; features a dedicated entrance to expedite law enforcement drop-off, taking officers about 10 minutes | Tucson, AZ | No Formal Evaluation | |
| CM (Contingency Management) | An evidence-based treatment primarily for stimulant use disorders (like cocaine or methamphetamine); uses incentives, often cash payments, for specific positive behaviors such as providing clean drug tests | General practice (e.g., San Francisco pilot) | Systematic Review Review finds CM to be an effective treatment for individuals with opioid use disorder. | |
| MAT (Medication-Assisted Treatment) | Utilizes medications like methadone or buprenorphine (Suboxone) to treat opioid use disorder; can include flexible take-home policies and delivery services to increase access and stability | General practice (e.g., San Francisco) | San Francisco Evaluation Evaluation finds that MAT reduces hospitalizations and improves stability. | |
| MAP (Managed Alcohol Use Program) | Stabilization and harm-reduction intervention for people with alcohol use disorder, sometimes involving managed alcohol programs where clients are given small amounts of alcohol; also known as "wet housing" | General practice (e.g., San Francisco) | Systematic Review Review finds MAPs a promising harm reduction intervention. | |
| Housing | ||||
| HRH (Harm Reduction Housing) | Provides stable living environments without sobriety mandates; offers 24/7 harm reduction supplies, counseling and medical oversight on-site to reduce the risks associated with drug use, such as using alone | Boston, MA | No Formal Evaluation | |
| Temporary Shelter Provision (Winter Shelter Beds) | Provision of additional temporary shelter capacity during the winter months | Los Angeles County, CA | Los Angeles Evaluation A study finds these programs reduce unsheltered homelessness as well as crime and ER visits. | |
| Tiny Cabins / Tiny Homes | Noncongregate, cost-effective interim housing options; San Francisco's first cabin community was established quickly on borrowed private land for temporary use | San Francisco, CA | No Formal Evaluation | |
| Justice Involved | ||||
| LEAD (Let Everyone Advance with Dignity) | Case management diversion for low-level offenses, replacing arrest with community-based care | Seattle, WA (replicated nationally) | North Carolina Evaluation Participants are less likely to have arrests and outpatient behavioral visits as well as higher utilization of medication. | |
Glossary of terms
Systems, agencies and programs
311/911 Systems
311/911 are the City’s call systems consisting of nonemergency (311) and emergency (911) dispatch lines, routing homeless concerns through 311 and psychiatric crises through 911.
988 is the City’s suicide and crisis call system, which can also dispatch DOHMH operated MCT teams to individuals in crisis.
AOT — Assisted Outpatient Treatment (Kendra’s Law)
AOT is authorized by a 1999 State law (Kendra’s Law), consists of court-ordered treatment plans and mandates medication, therapy and case management for individuals with severe illness and treatment noncompliance history. The petition can be filed by a range of individuals including a hospital director, psychiatrist, psychologist, probation officer or family members.
CIDI — Center for Innovation through Data Intelligence
CIDI is the Mayor’s Office data hub. It consists of integrated databases linking City systems and coordinates cross-agency data integration.
DHS — NYC Department of Homeless Services
DHS is the City agency that funds and operates shelter systems, street outreach providers and street outreach nurses, and manages temporary living (e.g., Safe Havens).
DOHMH — NYC Department of Health and Mental Hygiene
DOHMH is the City agency that operates behavioral health programs, deploys mobile crisis teams and coordinates mental health strategy with H+H and nonprofits.
H+H — NYC Health + Hospitals
H+H is the City’s public hospital system, which operates emergency departments, CPEPs, Correctional Health Services at Rikers and different treatment and transition programs (e.g., Just Home).
HUD — U.S. Department of Housing and Urban Development
HUD is the federal agency that funds housing vouchers and homelessness assistance programs including Continuum of Care and HUD-VASH.
MOCJ — Mayor’s Office of Criminal Justice
MOCJ is the mayor’s coordinating office for criminal justice policy. It manages diversion and reentry initiatives and oversees supportive housing programs for justice-involved individuals.
OASAS — Office of Addiction Services and Supports
OASAS is the New York State agency that funds and operates substance use treatment programs, funds harm reduction and recovery services and oversees addiction treatment policy statewide.
OMH — New York State Office of Mental Health
OMH is the New York State agency that funds and operates psychiatric programs and institutions and oversees mental health policy statewide.
OTDA — Office of Temporary and Disability Assistance
OTDA is the State agency that administers emergency aid programs, funds supportive housing grants and oversees temporary assistance policy.
SAMHSA — Substance Abuse and Mental Health Services Administration
SAMHSA is the federal agency that funds behavioral health block grants, supports State and local programs and sets national behavioral health policy.
VA — U.S. Department of Veterans Affairs
VA is the federal agency that operates veteran health facilities, runs HUD-VASH housing programs, and provides mental health services for veterans.
Crisis outreach and treatment programs
ACT — Assertive Community Treatment
ACT teams are operated by the New York State Office of Mental Health. They consist of psychiatrists, nurses, social workers and peer specialists, and provide 24/7 field-based treatment for adults with severe mental illness.
B-HEARD — Behavioral Health Emergency Assistance Response Division
B-HEARD is a City pilot program staffed by FDNY and H+H. It consists of unarmed clinician-EMT teams and responds to mental health 911 calls in select precincts.
CPEP — Comprehensive Psychiatric Emergency Program
CPEP are 24/7 psychiatric emergency programs funded by the State and operated by City hospitals, providing critical crisis and evaluation services to individuals with serious mental illness.
CTI - Critical Time Intervention
CTI, founded in New York City, is a time-limited, evidence-based case management model employed by SOS teams that provides intensive support during periods of transition for individuals in crisis and cycling between systems.
EOL — End of Line
EOL are multiagency teams working at end-of-line stations as part of the Subway Safety Plan, connecting individuals to services.
FACT — Forensic Assertive Community Treatment
FACT teams are a specialized ACT model. They consist of behavioral health clinicians and criminal justice liaisons and provide integrated treatment and supervision for people with serious mental illness involved in the justice system.
Free, voluntary, member-led spaces administered and run by Fountain House, serving adults with serious mental illness in New York City.
IMT — Intensive Mobile Treatment
IMT teams are operated by DOHMH. They consist of clinical staff similar to ACT composition and treat people with serious mental illness who are homeless, recently incarcerated or repeatedly hospitalized.
MCTs — Mobile Crisis Teams
MCTs are operated by DOHMH. They consist of clinician-led rapid-response units and respond to psychiatric crises dispatched through 988 or hospital networks.
Medical respite is funded by the State and operated by H+H, offering short-term medical respite beds for people exiting hospitals who are homeless.
PATH — Police and Transit Homelessness Co-response Program
PATH operates primarily overnight; consists of joint teams from NYPD, DHS and H+H; and responds to homelessness in subway and transit systems.
SCOUT — Subway Clinician Outreach Unit Teams
SCOUT operates primarily during daytime hours, consists of clinician-led teams partnered with MTA and DHS, and provides outreach in the subway system.
Situation Tables
Cross-agency meetings (police, clinicians, outreach, housing) reviewing the highest-risk individuals and coordinating targeted interventions.
SOS Teams — Safe Options Support
SOS teams are funded by OMH, consist of multidisciplinary outreach workers and conduct street outreach to connect unsheltered individuals to housing and other services.
Housing and shelter programs
JISH — Justice-Involved Supportive Housing
JISH is a housing model that consists of apartments with intensive supervision and clinical services both for justice-involved individuals with serious mental illness exiting jail or prison.
Safe Havens, funded and operated by DHS, are low-threshold residential housing for street homeless individuals. They consist of single rooms with reduced rules (pets allowed, no curfews, couples permitted) and serve a high-need population who decline traditional shelters.
Stabilization beds, funded and operated by DHS, are short-term, low-threshold beds for individuals transitioning from the street to more permanent housing. They are typically less service-intensive than Safe Havens.
Supportive housing is permanent affordable housing consisting of independent units with on-site case management and clinical services, and serving people with mental illness, disabilities or chronic homelessness.
Street-to-Housing is a pilot run by the Volunteers of America, consisting of single-room units with on-site supports to place individuals directly from the street into housing without shelter system entry.
Legal frameworks and mental hygiene laws
MHL 9.41 (Police Removal)
MHL 9.41 is a State mental hygiene law provision authorizing NYPD officers to transport individuals for psychiatric evaluation. It applies when someone poses danger to themselves or others or cannot meet basic needs.
MHL 9.58 (Clinical Removal)
MHL 9.58 is a State mental hygiene law provision authorizing licensed mental health professionals to order transport to hospitals. It applies under similar danger criteria as 9.41.
These are State psychiatric hospitalization statutes consisting of progressive commitment periods. They require escalating levels of clinical and judicial authorization:
- 9.40: Up to 72-hour evaluation
- 9.39: Up to 15-day emergency hospitalization
- 9.27 / 9.37: 60-day commitment with physician certification
- 9.33: Court-ordered extended hospitalization
Kendra’s Law is a 1999 State statute. It established AOT following a homicide by a person with untreated schizophrenia and authorizes court-ordered outpatient treatment.
AB 210 (California)
AB 210 is California legislation. It authorizes data sharing across health, housing and safety providers with confidentiality protections; it is cited as a model for cross-system coordination.
Data and coordination initiatives
CAPS — Coordinated Assessment and Placement System
CAPS, operated by New York City’s Continuum of Care (CoC), is the City’s internal database for matching individuals to supportive housing and other placements.
CoC — Continuum of Care
New York City’s CoC is the HUD-mandated coordination system that consists of City agencies and nonprofit providers. It allocates federal homelessness funding and organizes service delivery.
StreetSmart is DHS’ digital platform. It consists of a database tracking outreach contacts by name and records engagement and progress of unsheltered individuals.
SPOA — Single Point of Access
SPOA, operated by DOHMH, helps connect people with serious mental illness to the appropriate providers.
Top 50 lists are internal by-name rosters that identify the most vulnerable or frequently encountered individuals. They are used to prioritize interventions in subways and on streets.
Funding and contracting
Outcome-based contracting is a proposed payment model for New York City nonprofits. It ties funding to results like housing stability or reduced crisis recurrence and shifts from activity-based to results-based reimbursement.
Bundled payments are a proposed funding structure. They consist of single-payment streams covering all services for an individual (housing, care, outreach) and make one provider accountable for coordination.
Prompt Pay Standard
The prompt pay standard is a proposed contracting reform that requires timely payments to nonprofit providers and aims to prevent cash-flow crises that delay service delivery.
Clinical and behavioral concepts
SMI — Serious Mental Illness
SMI is a diagnosable mental, behavioral or emotional disorder — such as bipolar disorder, major depressive disorder and schizophrenia — that substantially interferes with a person’s life and ability to function.
Co-Occurring Disorders / Dual Diagnosis
“Co-occurring disorders” refers to concurrent mental illness and substance use disorder. Common among street homeless populations, co-occurring disorders require integrated treatment approaches.
Anosognosia is a psychiatric symptom consisting of lack of awareness of one’s own mental illness. It contributes to treatment refusal in disorders like schizophrenia.
Psychosis / Drug-Induced Psychosis
Psychosis is a mental state involving loss of contact with reality. It can be triggered or worsened by substance use and includes symptoms like hallucinations and delusions.
TBI — Traumatic Brain Injury
TBI is a neurological injury caused by external physical trauma to the head due to assault, falls and accidents, ranging from mild concussions to severe brain damage.
════════════════════════════════════════
New York is entering an historic and pivotal transition. Mayor-elect Mamdani faces big problems on housing, safety, mental health, transit, and more.
Vital City is uniquely positioned to offer clear, practical guidance rooted in evidence. Ideas that could actually be implemented and work.
But to meet this moment, we need to grow.
That’s why, this year, for the first time, we’re asking our readers to support Vital City directly. We’re aiming for 700 inaugural supporters by December 31.
Your support will help us expand our editorial capacity, strengthen our operational support, and continue delivering thoughtful, relevant and informative work in 2026.
If this article informed your thinking, challenged you, or helped you understand the city more clearly, please consider supporting the work behind it.
Make your tax-deductible gift and help us reach 700 supporters.



